Tranexamic Acid (TXA) — Detail
Cyklokapron · Lysteda (PO)
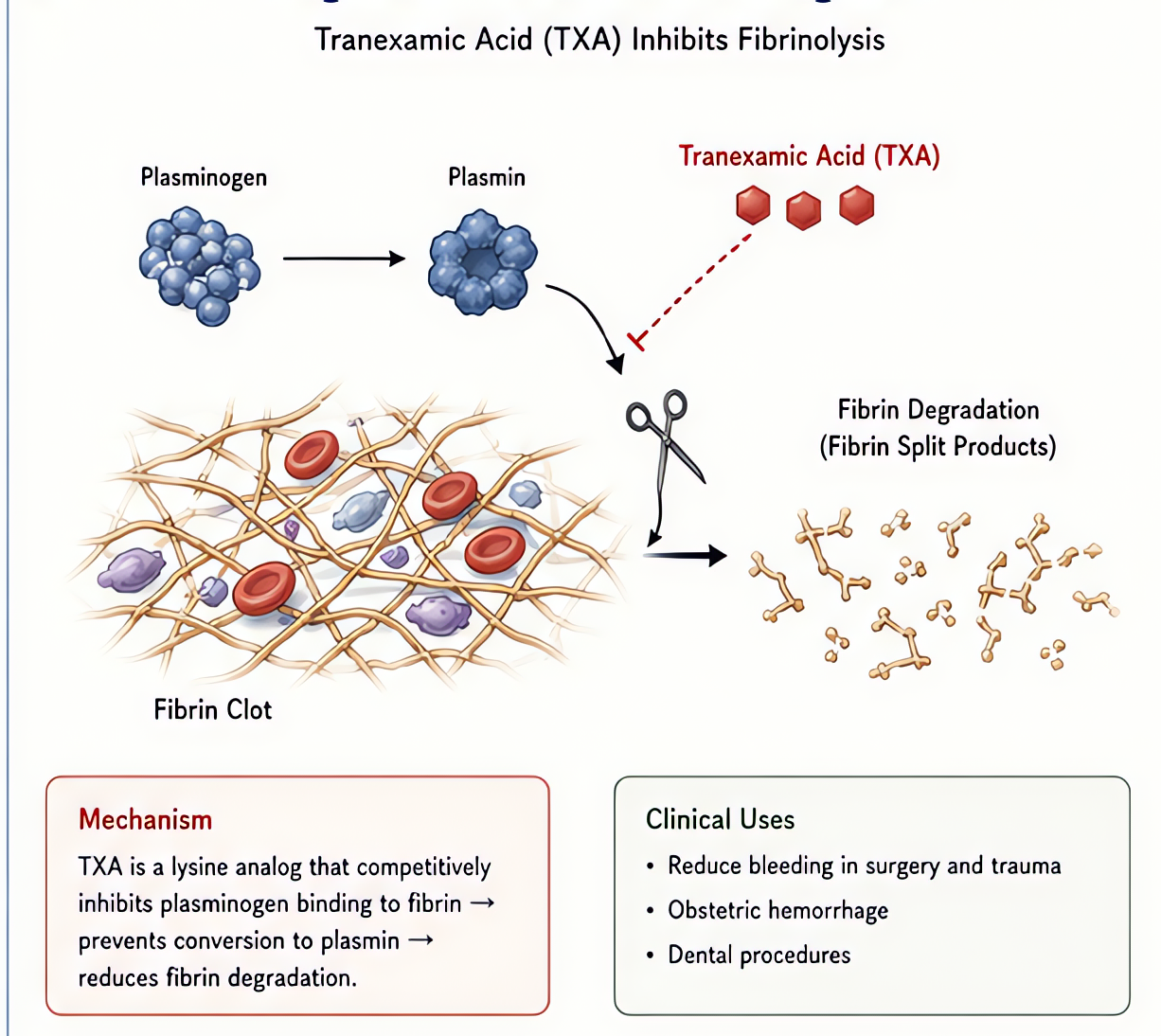
Antifibrinolytic / synthetic lysine analog
Synthetic lysine analog. Competitively binds plasminogen LYSINE binding sites, preventing plasminogen activation to plasmin. Inhibits fibrinolysis without inducing hypercoagulability per se.
Indications
- •Trauma hemorrhage (CRASH-2: 1g IV over 10 min + 1g over 8 h within first 3 h reduces all-cause mortality)
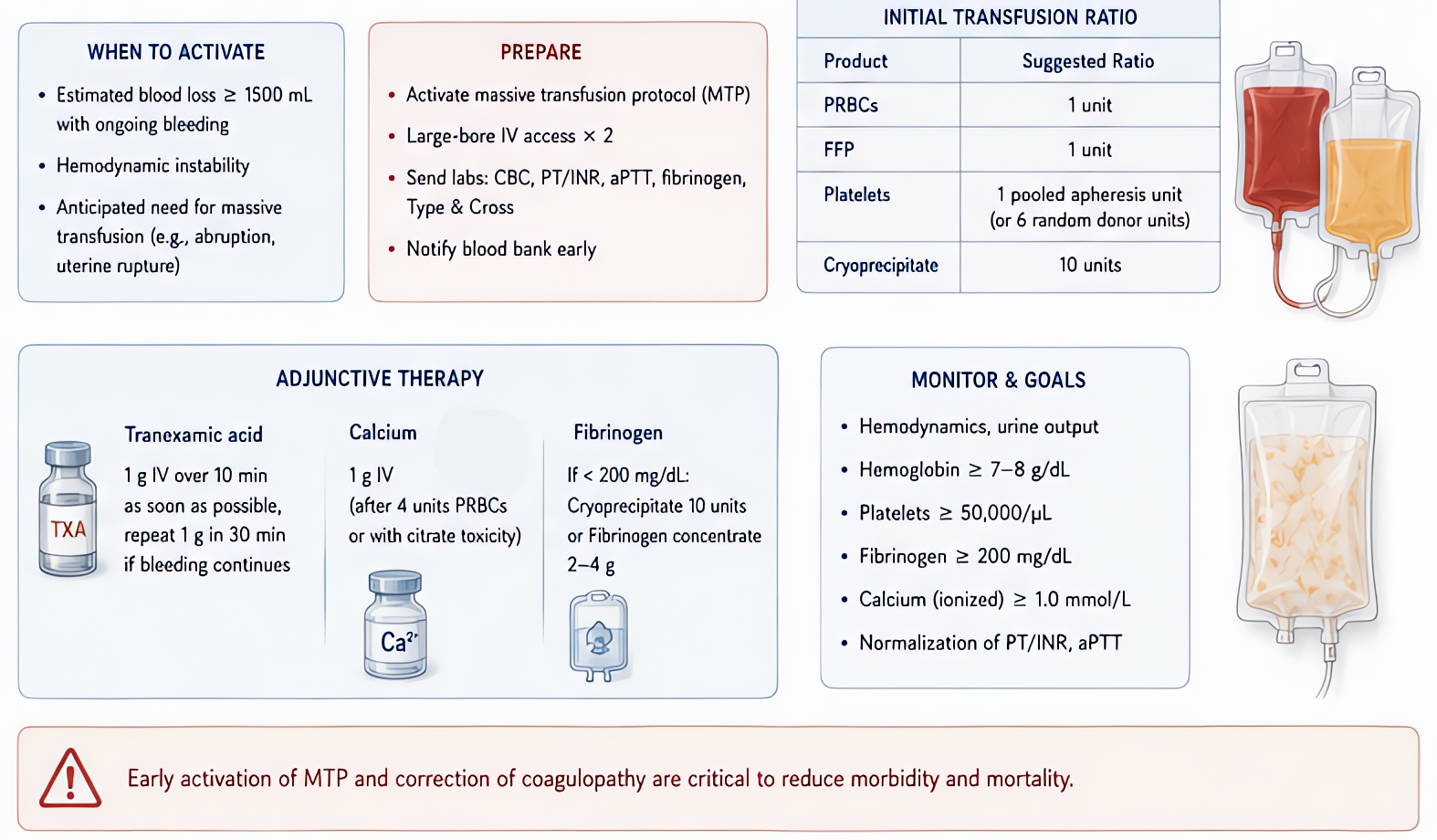
- •Postpartum hemorrhage (WOMAN trial: 1g IV reduces death from bleeding)
- •Cardiac surgery (reduces blood loss + transfusion)
- •Spine surgery, total joint, liver transplant
- •Hereditary angioedema prophylaxis
- •Heavy menstrual bleeding (PO formulation)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Trauma (CRASH-2) | 1 g IV over 10 min within FIRST 3 H of injury, then 1 g over 8 h | — |
| Postpartum hemorrhage (WOMAN) | 1 g IV over 10 min as soon as PPH diagnosed; can repeat 30 min later | — |
| Cardiac surgery | Loading 10-30 mg/kg IV + infusion 1-16 mg/kg/h | — |
| Spine/major ortho | 10-15 mg/kg IV at incision; some institutions add infusion | — |
| Topical (joint, surgical field) | 1-3 g in 100-200 mL saline applied topically | — |
| Pediatric (e.g. congenital cardiac) | (weight-based) | 10 mg/kg IV at induction + 1 mg/kg/h infusion |
Pharmacokinetics
Onset 5-10 min IV. Half-life ~2-3 h. Renal excretion >95% unchanged.
Hemodynamic effects
Hemodynamically neutral. Rapid IV bolus may cause transient hypotension or visual disturbances — give over 10 min for 1 g dose.
Side effects
- !Visual disturbances + hypotension (rapid bolus) — give over ≥10 min
- !Seizures (high-dose cardiac surgery — TXA is GABAA antagonist; reduce dose with CSF leak / BBB disruption)
- !Theoretical thromboembolism increase — meta-analyses show no clear increase
- !GI upset (PO)
- !Headache + nausea
Contraindications
- ×Active intravascular thrombosis (PE, DVT being treated)
- ×Subarachnoid hemorrhage (some debate)
- ×Severe renal impairment (dose reduction)
- ×Acute color vision deficit
Clinical pearls
- ★TIMING for trauma: 1 g WITHIN 3 HOURS reduces mortality. After 3 hours, NOT beneficial and may HARM.
- ★PPH: 1 g IV as soon as diagnosed; can repeat 30 min later.
- ★CARDIAC SURGERY: reduces bleeding + transfusion ~25%. Seizure risk at high-dose protocols (>50 mg/kg) — modern dose more conservative (10-30 mg/kg).
- ★SPINE SURGERY: 15 mg/kg IV at incision is standard — reduces blood loss + transfusion in scoliosis + multilevel fusion.
- ★TOPICAL: 1-3 g in saline applied to surgical wound (knee, hip) reduces bleeding without systemic exposure.
- ★Approximately $5-10 per dose IV — extreme cost-effectiveness.
Other drugs in Cardiac / BP
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
- Amiodarone
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert