Amiodarone
Cordarone · Pacerone · Nexterone
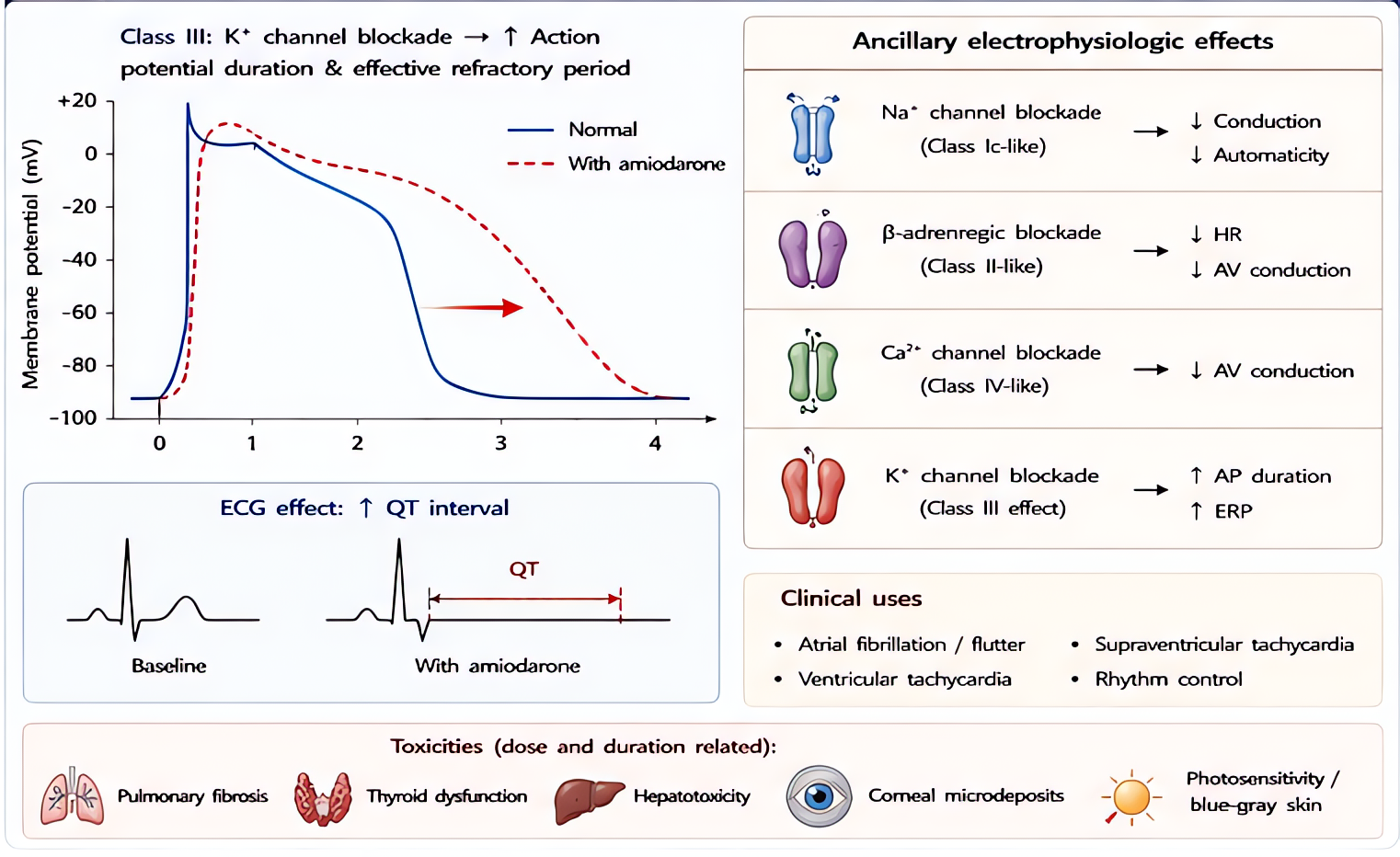
Class III antiarrhythmic (multichannel: K, Na, Ca, β-blocker)
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
Indications
- •Refractory VF/pulseless VT during cardiac arrest (after CPR + 1st defib + epi)
- •Stable monomorphic VT
- •Atrial fibrillation/flutter rate + rhythm control (when other agents fail)
- •Recurrent ICD shocks
- •Supraventricular tachycardia
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Cardiac arrest VF/pulseless VT | 300 mg IV bolus, then 150 mg q3–5 min × 1 (max 2.2 g/24 h) | — |
| Stable VT/AF | 150 mg IV over 10 min, then 1 mg/min × 6 h, then 0.5 mg/min × 18 h | — |
| Pediatric pulseless VT/VF | 5 mg/kg IV bolus | |
| Pediatric stable VT | 5 mg/kg IV over 20–60 min, may repeat to 15 mg/kg/day |
Pharmacokinetics
IV onset minutes; full effect hours to days. Massive volume of distribution (highly lipophilic — accumulates in fat, liver, lung). Half-life 25–110 days (chronic). Hepatic CYP metabolism, biliary excretion. Multiple drug interactions via CYP3A4 inhibition.
Hemodynamic effects
Modest hypotension (vasodilation from solvent excipient + Ca²⁺ blockade); bradycardia; minimal direct inotropy reduction. Less negative inotropy than other Class III antiarrhythmics. Older formulations (with polysorbate 80) cause more hypotension than aqueous Nexterone.
Side effects
- !ACUTE: hypotension (bolus too fast), bradycardia, AV block
- !Pulmonary fibrosis (chronic — 5–15% of long-term users)
- !Hepatotoxicity (chronic — LFT elevation)
- !Thyroid: hypo OR hyperthyroidism (iodine content 37%)
- !Corneal microdeposits (asymptomatic, common)
- !Photosensitivity, blue-gray skin discoloration
- !QT prolongation (rare TdP given multichannel effect)
Contraindications
- ×2nd/3rd degree AV block (without pacemaker)
- ×Sinus node dysfunction with bradycardia
- ×Cardiogenic shock (relative)
- ×Iodine allergy (rare; cross-reactivity uncommon but documented)
Clinical pearls
- ★Code dose: 300 mg IV push for VF/pulseless VT after 1st defibrillation + epinephrine (per AHA ACLS).
- ★DILUTION: bolus must be diluted (5% dextrose for older formulation; aqueous Nexterone OK in either D5 or NS) — undiluted causes severe phlebitis.
- ★AF cardioversion: 150 mg load + infusion; conversion can take hours. Patient should already be anticoagulated if AF >48 h (TEE-guided alternative).
- ★DRUG INTERACTIONS via CYP3A4 inhibition: warfarin (↑INR), digoxin (↑levels — halve dose), simvastatin (rhabdo), amiodarone affects nearly everything chronic patients take.
- ★Postop new AF in cardiac surgery: amiodarone 150 mg load + 1 mg/min × 6 h often works when β-blockade doesn't.
- ★Use Nexterone (aqueous, sulfobutylether-β-cyclodextrin solubilizer) over older Cordarone for HD-stable patients — less hypotension on bolus.
Other drugs in Cardiac / BP
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
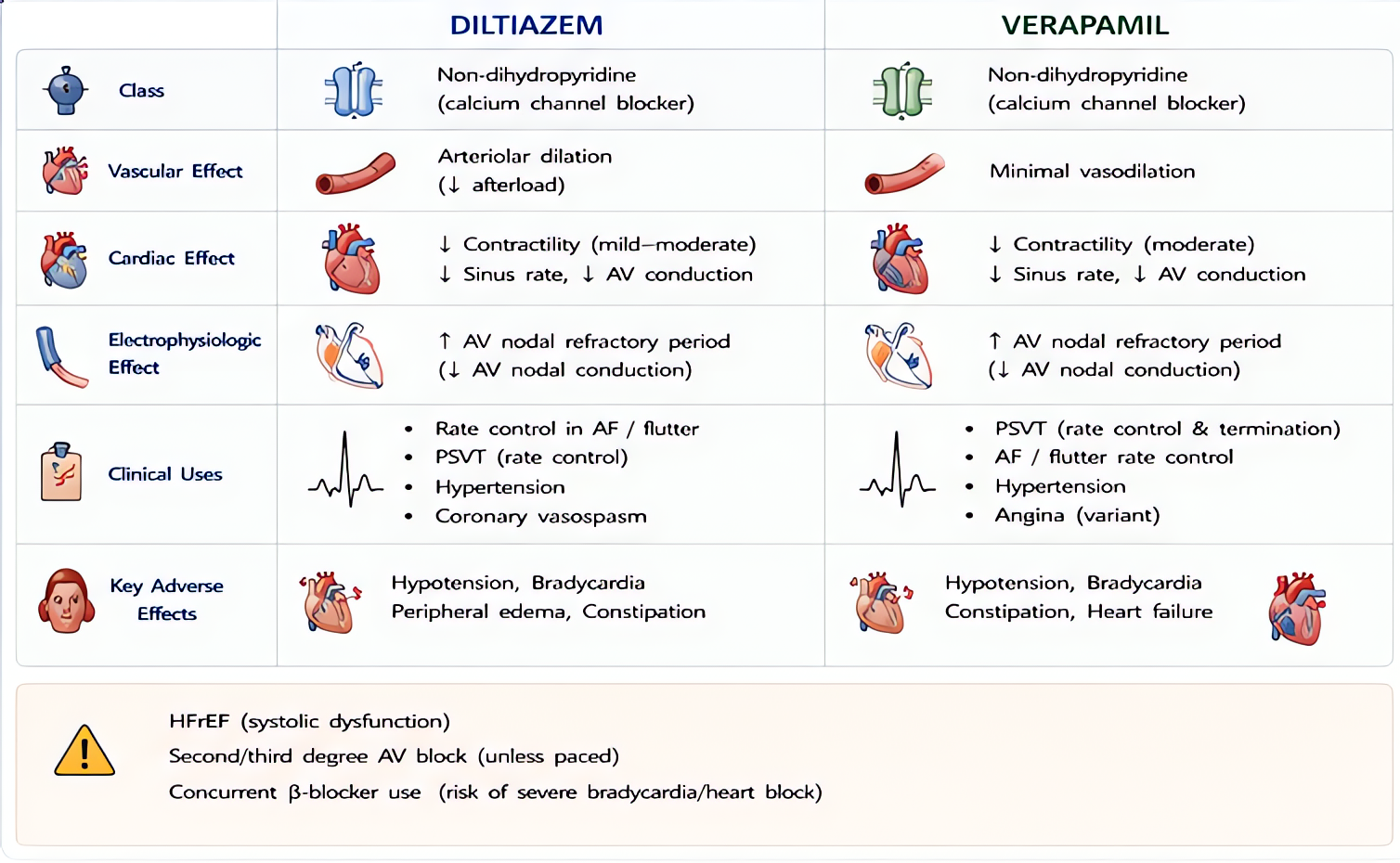
- Nicardipine
Selective L-type voltage-gated calcium channel blocker, dihydropyridine class (vascular >> cardiac selectivity). Vascular smooth muscle relaxation → arterial vasodilation → afterload reduction. Minimal direct cardiac inotropic or chronotropic effect at clinical doses (vs verapamil/diltiazem which are non-selective).
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert
- •AHA ACLS guidelines, 2020