Norepinephrine
Levophed
Endogenous catecholamine, α1 > β1 agonist
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
Indications
- •Septic shock (first-line)
- •Vasoplegic shock post-bypass
- •Distributive shock
- •Anesthesia-induced hypotension (refractory)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Infusion | 0.01–1 mcg/kg/min (titrated to MAP) | — |
Pharmacokinetics
Onset seconds. Duration < 5 min after infusion stop.
Hemodynamic effects
↑SVR, ↑BP, slight ↑CO. Reflex bradycardia rare.
Side effects
- !Distal ischemia (digits, mesenteric — especially with high-dose, prolonged)
- !Extravasation necrosis — treat with phentolamine
- !Reduced renal/splanchnic perfusion at high dose
Contraindications
- ×Hypovolemic shock without volume resuscitation (relative)
Clinical pearls
- ★Surviving Sepsis: NE first-line, MAP target ≥ 65.
- ★Central line preferred but a peripheral 18g + close monitoring acceptable for short courses (recent literature).
Other drugs in Cardiac / BP
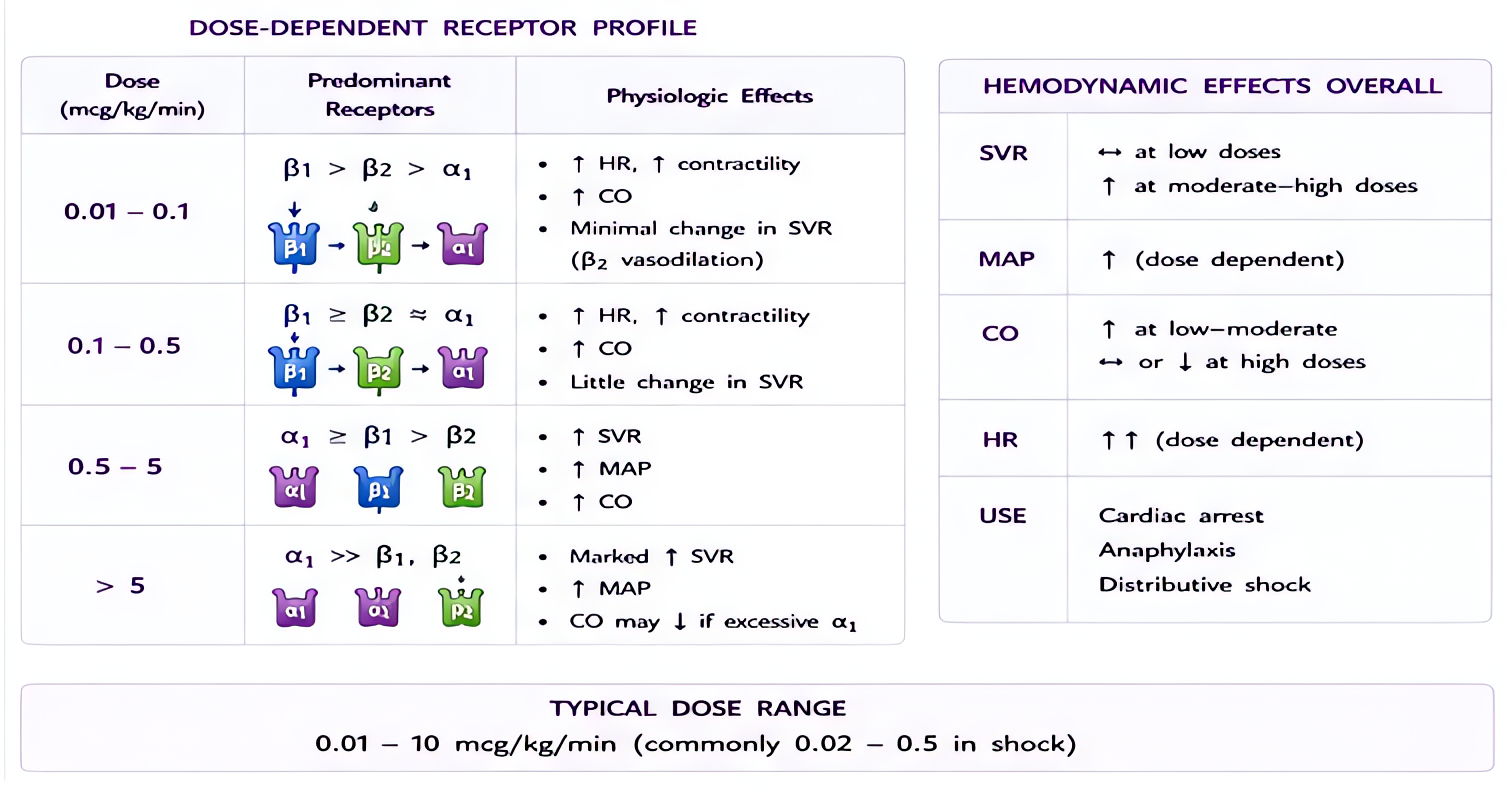
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
- Amiodarone
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
- Nicardipine
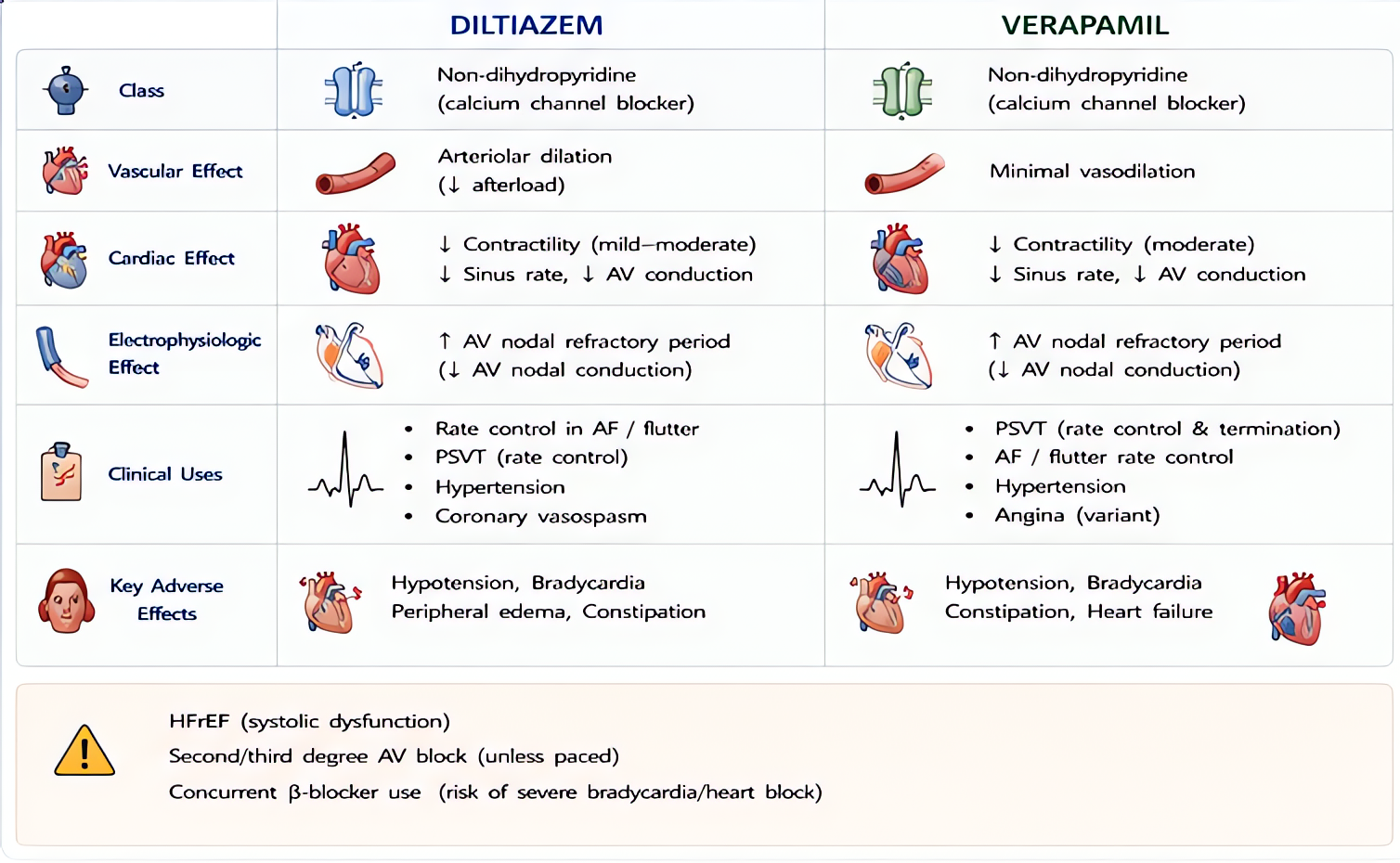
Selective L-type voltage-gated calcium channel blocker, dihydropyridine class (vascular >> cardiac selectivity). Vascular smooth muscle relaxation → arterial vasodilation → afterload reduction. Minimal direct cardiac inotropic or chronotropic effect at clinical doses (vs verapamil/diltiazem which are non-selective).
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert