Nitroglycerin
Nitrostat · Nitro-Bid
Organic nitrate / nitric oxide donor / vasodilator
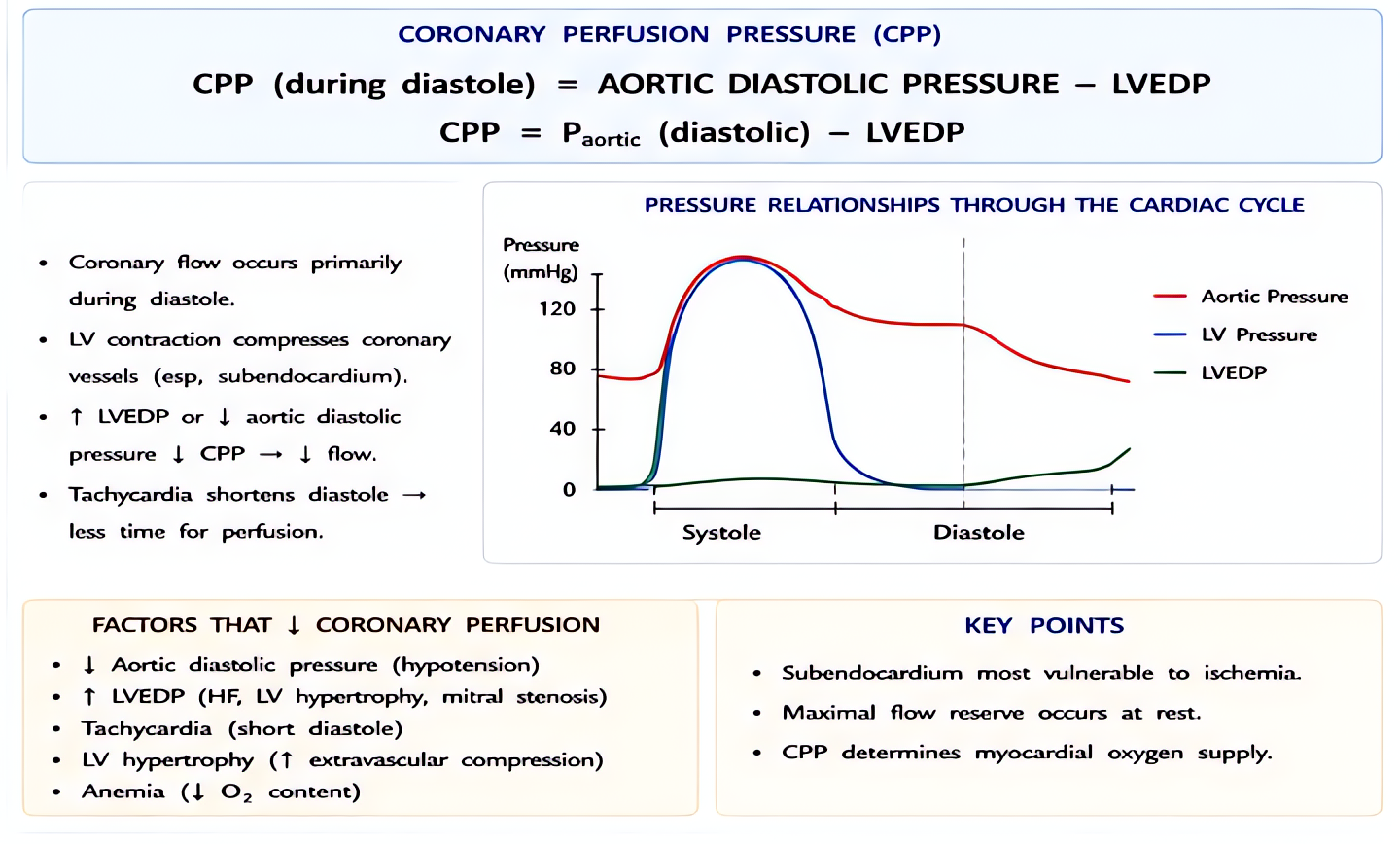
Metabolized to nitric oxide (NO) in vascular smooth muscle → activates guanylyl cyclase → ↑cGMP → smooth muscle relaxation. PREFERENTIAL VENOUS dilation (low doses) → reduces preload (decreases LV wall stress, ↓myocardial O₂ demand). Higher doses → arterial dilation, including coronary arteries (↑coronary perfusion in non-stenotic vessels).
Indications
- •Angina/MI (chronic, acute)
- •Acute LV failure / pulmonary edema
- •Controlled hypotension intraop (rare modern use)
- •Coronary vasospasm (Prinzmetal)
- •Esophageal achalasia (acute relaxation of lower esophageal sphincter)
- •Pulmonary hypertension acute management
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Sublingual angina | 0.4 mg SL q5min × 3 | — |
| Continuous infusion (acute MI, HF, controlled hypotension) | 5-200 mcg/min IV titrated to target | — |
| Bolus IV (esophageal spasm, sphincter relaxation) | 50-200 mcg IV | — |
| Topical paste | 1-2 inches q4-6h chronic | — |
Pharmacokinetics
Onset 1-3 min IV. Half-life 1-3 min (very short). Hepatic metabolism via glutathione + organic nitrate reductase. Tachyphylaxis develops within 24 h continuous infusion (sulfhydryl depletion) — drug-free interval needed for chronic use.
Hemodynamic effects
↓Preload (dominant low dose), ↓afterload (high dose), reflex tachycardia possible, may lower coronary perfusion pressure (if MAP drops disproportionately). At low/moderate dose: improves coronary supply > increases demand.
Side effects
- !Hypotension (additive with other antihypertensives)
- !Headache (universal — common reason for non-compliance)
- !Methemoglobinemia (rare, with very high cumulative doses)
- !Tachyphylaxis with continuous infusion >24 h
- !Reflex tachycardia
Contraindications
- ×Hypotension (already low BP)
- ×Severe aortic stenosis (preload reduction → severe hypotension)
- ×Right ventricular MI (preload-dependent state)
- ×Concurrent PDE5 inhibitor (sildenafil, tadalafil) — severe hypotension within 24-48 h of use
- ×Increased ICP (cerebral vasodilation)
- ×Constrictive pericarditis (preload-dependent)
Clinical pearls
- ★FIRST-LINE for myocardial ischemia + acute LV failure — preload reduction often resolves both.
- ★PDE5 inhibitor (sildenafil, tadalafil) within 24 h: avoid nitroglycerin — severe refractory hypotension via additive cGMP elevation.
- ★INFERIOR/RV MI: AVOID — preload-dependent state, NTG drops preload → severe hypotension. Use cautiously.
- ★Controlled hypotension: nicardipine + esmolol preferred over NTG in modern practice (NTG tachyphylaxis + tachycardia limit titration).
- ★Concentration: standard intraop infusion 100 mcg/mL (50 mg in 500 mL D5W). Start 10-20 mcg/min, titrate to target. Avoid PVC tubing — NTG adsorbs (use polyolefin/polyethylene tubing).
- ★Esophageal spasm or sphincter relaxation: 50-200 mcg IV bolus rapidly relaxes (ENT useful adjunct for vocal cord adduction during awake fiberoptic too).
Other drugs in Cardiac / BP
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
- Amiodarone
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert