Ephedrine
(generic)
Indirect + direct mixed alpha + beta sympathomimetic
Indirect-acting sympathomimetic — promotes release of stored norepinephrine from presynaptic vesicles AND has direct alpha + beta receptor agonism. Mixed action → increases HR (β1) + contractility (β1) + SVR (α1). Tachyphylaxis develops with repeated dosing (depleted NE stores).
Indications
- •Hypotension during anesthesia, especially with bradycardia (treats both HR + BP)
- •Hypotension after spinal/epidural anesthesia (alternative to phenylephrine, especially in non-OB)
- •Symptomatic hypotension in cardiac surgery (vasoconstrictor + inotropic support)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Hypotension bolus | 5–10 mg IV; can repeat q3–5 min (max ~50 mg/session before tachyphylaxis) | 0.1–0.2 mg/kg IV; can repeat q3–5 min |
| IM bolus (no IV) | 25–50 mg IM | 0.5 mg/kg IM |
Pharmacokinetics
Onset 1-2 min IV. Duration 10-15 min. Renal excretion (~95% unchanged). Half-life 3-6 h. Crosses placenta (use during cesarean — historical concern about fetal acidemia at high doses, but practically OK at standard doses).
Hemodynamic effects
↑HR, ↑contractility, ↑SVR → ↑BP. Useful for hypotension + bradycardia (in contrast to phenylephrine which is pure alpha → may cause reflex bradycardia).
Side effects
- !Tachycardia (problematic in CAD, AS)
- !Tachyphylaxis (depletion of stored norepinephrine)
- !Hypertension overshoot if dosed too aggressively
- !Catecholamine-like effects: tremor, anxiety in awake patient
- !Possible MI in susceptible patients (catecholamine-driven)
Contraindications
- ×Tachyarrhythmia
- ×Severe HTN, pheochromocytoma (uncontrolled catecholamine surge)
- ×Concurrent MAOI use (severe HTN crisis)
Clinical pearls
- ★FIRST-LINE for hypotension WITH BRADYCARDIA in non-OB cases — treats both HR + BP. If hypotension WITHOUT bradycardia or with tachycardia, phenylephrine is preferred.
- ★Cesarean spinal hypotension: PHENYLEPHRINE infusion is preferred over ephedrine boluses (Ngan Kee Anesth Analg 2010 — less fetal acidemia). Ephedrine has fallen from first-line in OB.
- ★TACHYPHYLAXIS: after 3-4 boluses, switch to phenylephrine or norepinephrine (works on different mechanism — direct receptor agonism unaffected by NE depletion).
- ★MAOI patients: indirect-acting sympathomimetics → catecholamine SURGE (norepinephrine pool not metabolized normally) → severe HTN crisis. Use direct-acting (phenylephrine, norepinephrine) instead.
- ★Standard concentration: 50 mg/mL ampoule; dilute to 5 mg/mL in saline (1 mL bolus) for routine intraop use.
Other drugs in Cardiac / BP
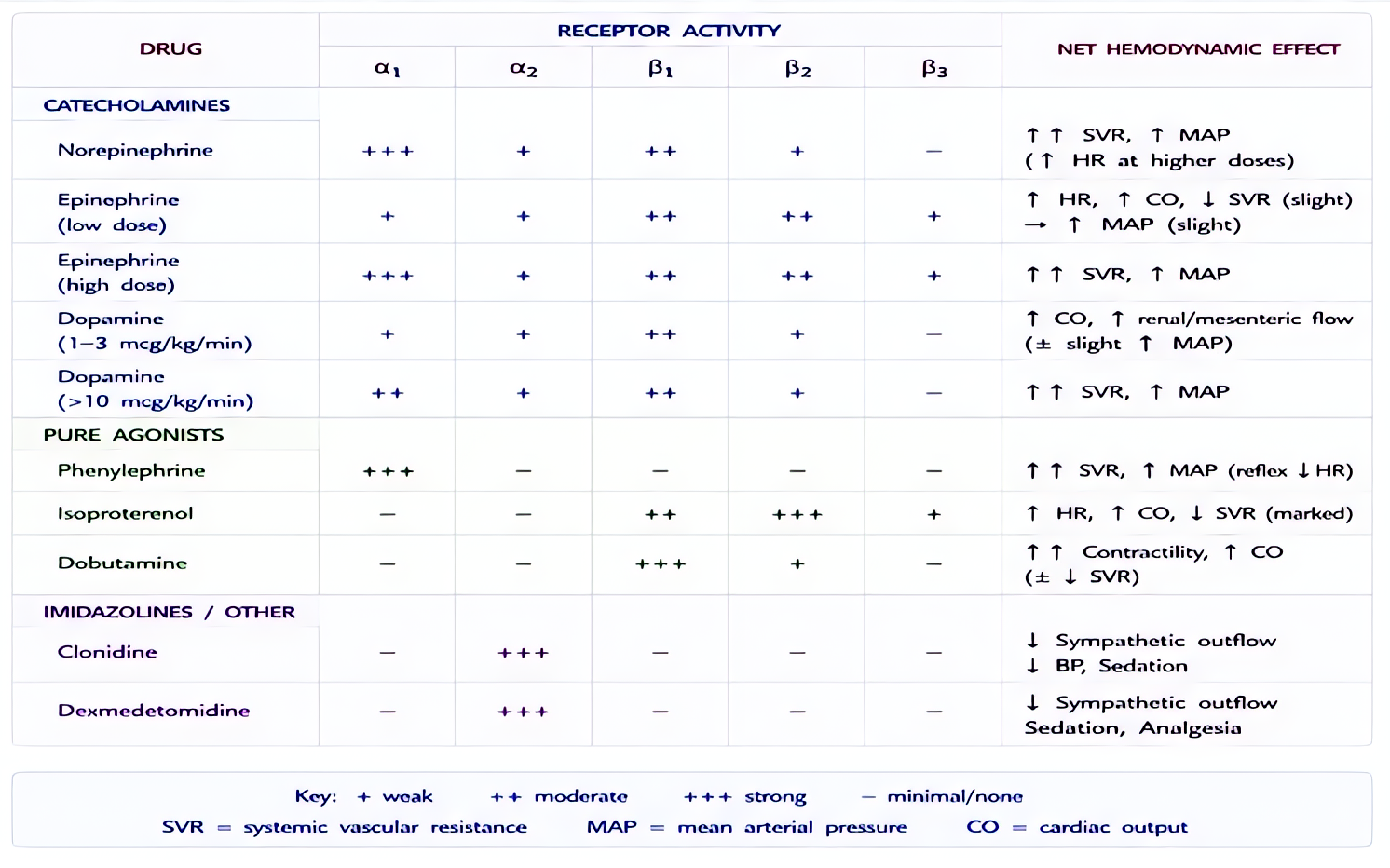
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
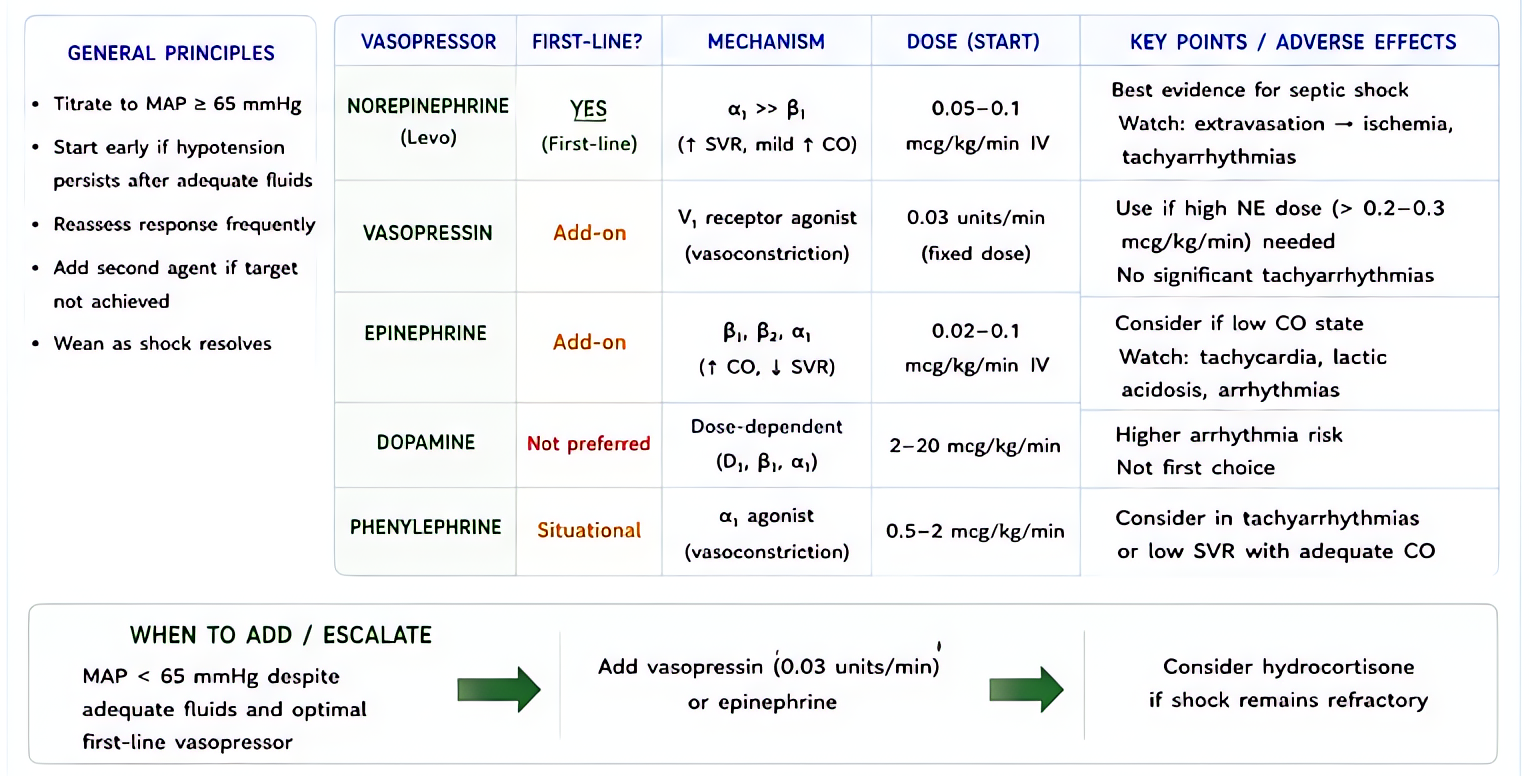
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
- Amiodarone
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert