Dobutamine
Dobutrex
Beta-1-selective synthetic catecholamine
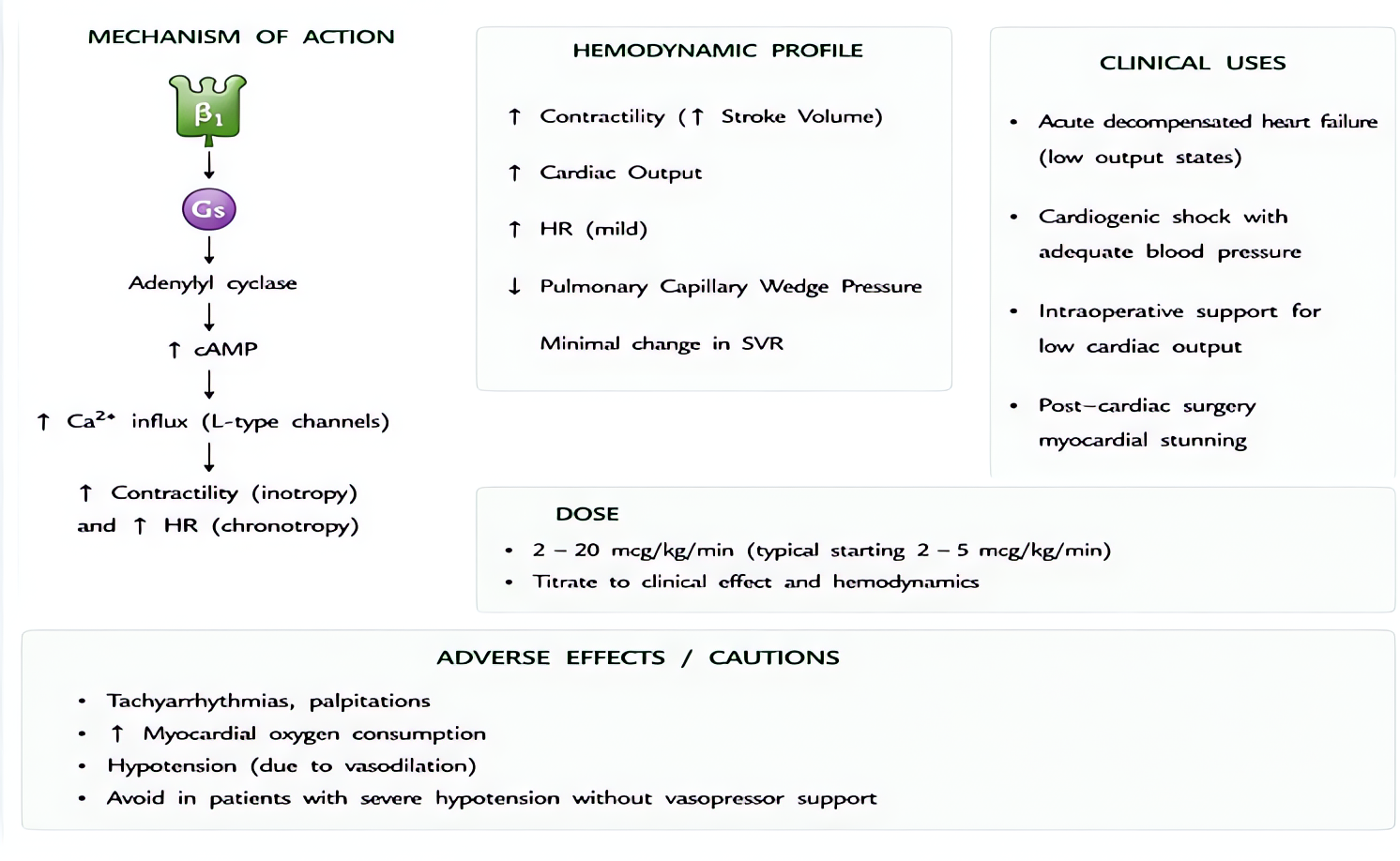
Synthetic catecholamine with PREDOMINANT β1 activity (also β2, mild α1). Pure inotrope — increases contractility + heart rate (β1) with mild vasodilation (β2 + α1 balance). Does NOT release endogenous norepinephrine (unlike ephedrine).
Indications
- •Cardiogenic shock with low cardiac output
- •Acute decompensated heart failure
- •Stress echocardiography (pharmacologic)
- •Bridge to LVAD or transplant
- •Septic shock with myocardial dysfunction (after norepinephrine)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Standard inotropic infusion | 2.5-20 mcg/kg/min IV titrated to CO/MAP | — |
| Pediatric | (weight-based) | 2.5-20 mcg/kg/min IV |
| Stress echo | 5-40 mcg/kg/min IV in graded steps | — |
Pharmacokinetics
Onset 1-2 min IV. Half-life ~2 min. COMT metabolism + renal excretion. Very predictable kinetics — easy to titrate.
Hemodynamic effects
↑Contractility, ↑HR (modest), ↑CO. BP variable — modest ↑MAP from increased CO offset by mild β2 vasodilation. ↓PVR. ↓SVR mildly.
Side effects
- !Tachycardia (more than milrinone)
- !Increased myocardial O2 demand (rate-related)
- !Atrial + ventricular arrhythmias
- !Tachyphylaxis with continuous infusion >72 h (β-receptor downregulation)
- !Hypotension at very high doses (β2 dominates)
Contraindications
- ×Severe AS (relative)
- ×Hypertrophic obstructive cardiomyopathy
- ×Tachyarrhythmia
- ×Pheochromocytoma
Clinical pearls
- ★FIRST-LINE inotrope for cardiogenic shock when MAP adequate (need norepinephrine added if hypotension).
- ★Vs milrinone: SHORTER half-life (~2 min vs ~2 h) — easier to titrate, faster wash-out, more predictable. But more tachycardia/arrhythmia.
- ★Pulmonary HTN: less PVR reduction than milrinone — milrinone preferred for RV failure with high PVR.
- ★Sepsis: NOREPINEPHRINE first; ADD dobutamine if low CO + adequate MAP after norepi (Surviving Sepsis 2021).
- ★Stress echo: 5 mcg/kg/min start, increase q3 min to max 40 + atropine if HR doesn't reach 85% age-predicted.
Other drugs in Cardiac / BP
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert