Plasma-Lyte 148 (and similar balanced solutions)
Plasma-Lyte 148 · Normosol-R · Isolyte E
Balanced calcium-free isotonic crystalloid
Na⁺ 140, Cl⁻ 98, K⁺ 5, Mg²⁺ 3, acetate 27, gluconate 23 mEq/L; osmolality 294 mOsm/kg. Acetate and gluconate metabolize independent of liver perfusion (unlike lactate), making it useful in liver failure / shock states. No calcium → fully compatible with blood products.
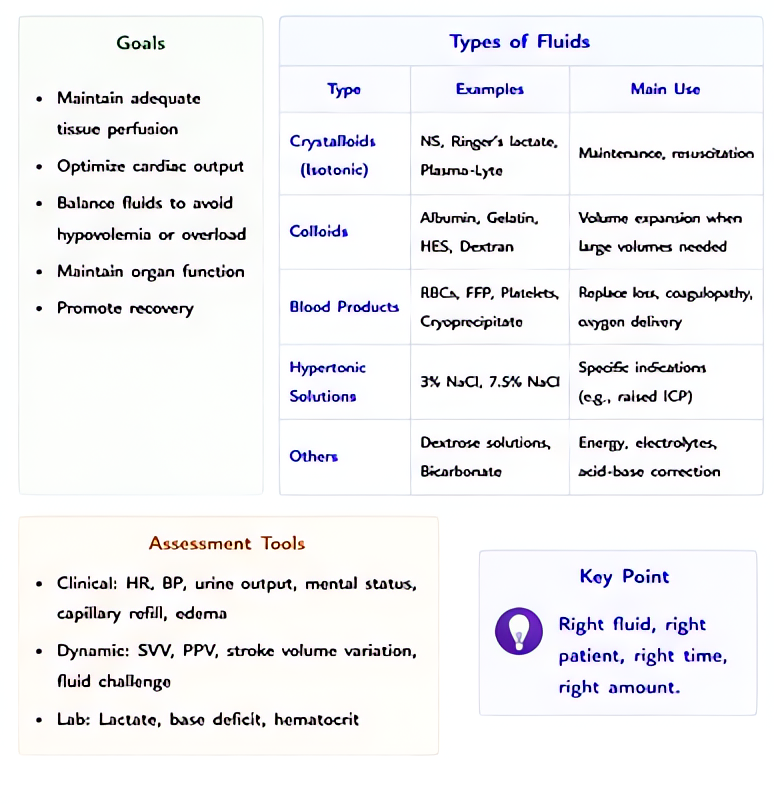
Indications
- •Balanced resuscitation when calcium-free fluid preferred (running with blood products, hepatic failure)
- •Sepsis resuscitation
- •Trauma resuscitation
- •Surgical maintenance
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Resuscitation bolus | 500–1000 mL IV | 10–20 mL/kg |
| Maintenance | 1–2 mL/kg/h surgical | — |
Pharmacokinetics
Acetate metabolized by skeletal muscle (much faster than hepatic lactate metabolism — useful in liver failure and shock).
Hemodynamic effects
Volume expansion; minimal direct effect.
Respiratory effects
Pulmonary edema with over-resuscitation.
Side effects
- !Volume overload
- !Mild metabolic alkalosis at large volumes (acetate metabolism generates HCO₃⁻)
Contraindications
- ×Hyperkalemia (relative — same K⁺ content as LR)
- ×Hypermagnesemia (relative)
Clinical pearls
- ★BLOOD COMPATIBILITY: no calcium → fully compatible with PRBC/FFP/platelets through the same line. This is Plasmalyte's main edge over LR in massive transfusion.
- ★SHOCK / LIVER FAILURE: acetate is metabolized in skeletal muscle, not liver — better buffering in shock liver, hepatic failure, or post-transplant patients than LR's hepatic-dependent lactate.
- ★BaSICS TRIAL (JAMA 2021): in 11,000 ICU patients, Plasma-Lyte vs 0.9% saline showed no 90-day mortality difference. Combined with PLUS (NEJM 2022, similar null result), the SMART/SALT-ED balanced-fluid signal weakened — current 2024 consensus is balanced is reasonable default but harm of saline likely overstated.
- ★OSMOLALITY 294: closer to plasma than LR's 273 — small theoretical edge in TBI but no head-to-head data; LR is still typically avoided in confirmed TBI in favor of NS.
- ★COST + AVAILABILITY: Plasmalyte costs more than LR. Most systems use LR as default balanced fluid; Plasmalyte for blood-product-compatibility scenarios.
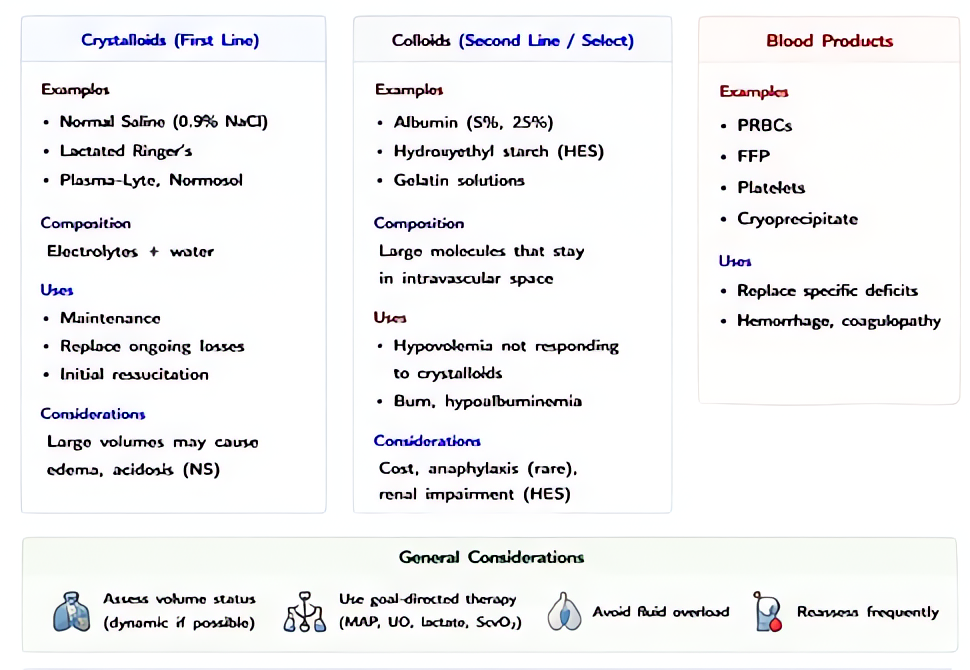
Other drugs in Crystalloids
- Normal Saline (0.9% NaCl)
0.9% sodium chloride in water — Na⁺ 154 mEq/L, Cl⁻ 154 mEq/L, osmolality 308 mOsm/kg. Distributes throughout the extracellular space; ~25–30% of infused volume remains intravascular at 30–60 min.
- Lactated Ringer's (LR / Hartmann's solution)
Na⁺ 130, Cl⁻ 109, K⁺ 4, Ca²⁺ 3, lactate 28 mEq/L; osmolality 273 mOsm/kg (slightly hypotonic). Lactate metabolized by liver to bicarbonate, providing buffering. Closer to plasma electrolyte composition than saline.
- D5W (5% Dextrose in Water)
5% dextrose (50 g/L) in water — when dextrose is metabolized, the remaining solution is free water. Effectively a free-water source distributed across total body water (28–42 L in adult).
- Hypertonic Saline 3% (and 23.4%)
3% NaCl: Na⁺ 513 mEq/L, osmolality 1027 mOsm/kg. 23.4% NaCl: Na⁺ 4000 mEq/L. Pulls water from brain parenchyma across an intact blood-brain barrier into the intravascular space — reduces ICP and treats severe hyponatremia.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e