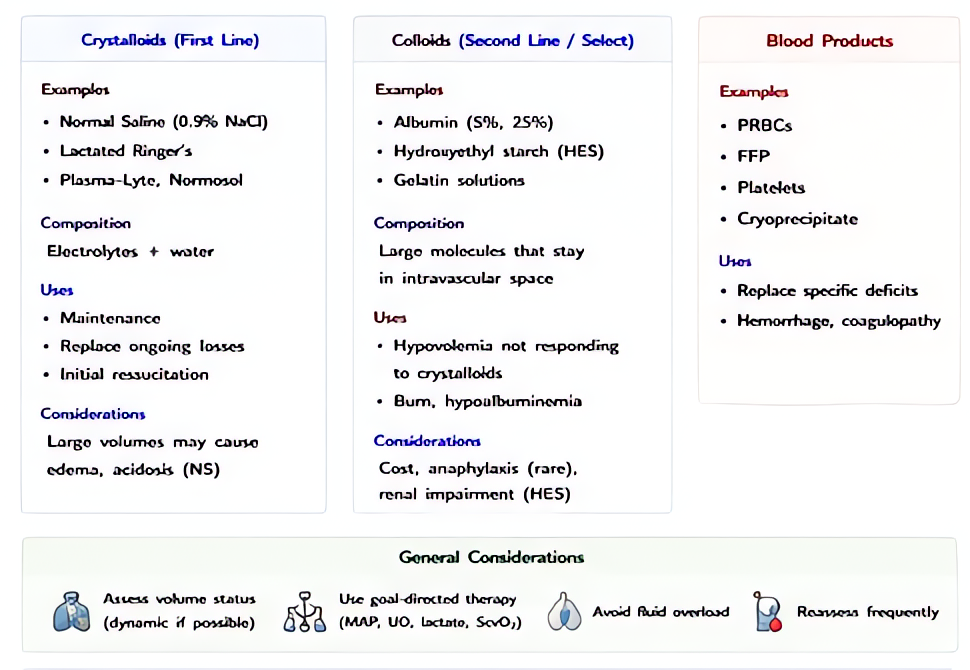
Normal Saline (0.9% NaCl)
NS · 0.9% sodium chloride
Isotonic non-balanced crystalloid
0.9% sodium chloride in water — Na⁺ 154 mEq/L, Cl⁻ 154 mEq/L, osmolality 308 mOsm/kg. Distributes throughout the extracellular space; ~25–30% of infused volume remains intravascular at 30–60 min.
Indications
- •Volume resuscitation when isotonic non-balanced fluid is required (hypochloremic metabolic alkalosis from vomiting/NGT, hyponatremia, traumatic brain injury — favored over LR)
- •Compatible carrier with blood products (LR's calcium can chelate citrate-bound transfusion citrate, theoretically; modern tubing rates make this near-irrelevant in practice)
- •Diluent for many IV medications
- •Initial fluid in DKA before switching to half-normal saline
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Volume resuscitation bolus | 500–1000 mL IV over 10–30 min, repeat as indicated | 10–20 mL/kg IV bolus |
| Maintenance | Holliday-Segar: 4 mL/kg/h first 10 kg + 2 mL/kg/h next 10 kg + 1 mL/kg/h thereafter; usually as 0.45% saline + dextrose, not full NS | — |
Pharmacokinetics
Distributes across extracellular space (~14 L in adult). 25–30% remains intravascular at 30 min. Renal excretion of excess Na/Cl.
Hemodynamic effects
Volume expansion; minimal direct effect.
Respiratory effects
Pulmonary edema possible with over-resuscitation.
Side effects
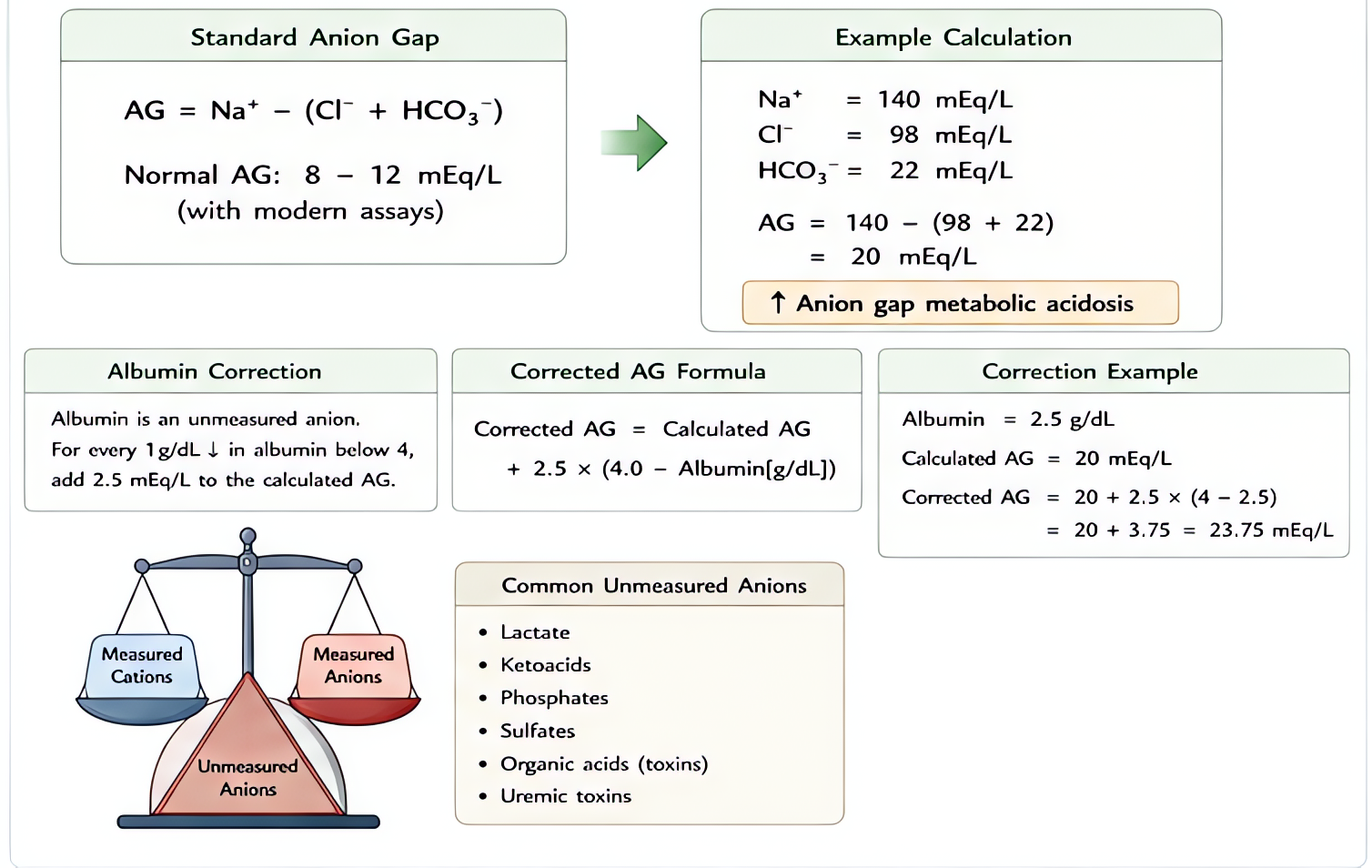
- !Hyperchloremic non-anion-gap metabolic acidosis at large volumes (>2–3 L) — driven by chloride load
- !Acute kidney injury (signal in SMART, SALT-ED — modest but reproducible)
- !Volume overload
- !Hypernatremia / dilutional hyponatremia depending on starting state
Contraindications
- ×Severe hyperchloremic acidosis
- ×Hypernatremia (relative)
- ×Heart failure with severe fluid restriction
Clinical pearls
- ★SMART TRIAL (NEJM 2018, Semler): in 15,000 ICU patients, balanced crystalloids (LR/Plasmalyte) reduced 30-day major adverse kidney events by 1.1% absolute vs saline. In SALT-ED, similar effect in non-ICU. SMART's effect was strongest in sepsis.
- ★TRAUMA / TBI FAVOR SALINE: hypotonic LR (273 mOsm) can theoretically worsen cerebral edema. NS (308 mOsm) preferred in confirmed or suspected TBI.
- ★DKA: NS first liter, then switch to 0.45% NS once Na corrected — gives more free water.
- ★HYPERCHLOREMIC ACIDOSIS: 0.9% saline has 154 Cl⁻; normal serum Cl⁻ is 95–105. Each liter pushes serum chloride up by ~3 mEq/L, generating a non-AG metabolic acidosis. Switch to balanced after 2–3 L.
- ★HYPERKALEMIA MYTH: NS is NOT preferred over LR in hyperkalemia. LR's 4 mEq/L K⁺ does not raise serum K⁺ in clinically relevant amounts (Khajavi 2008; O'Malley 2005). Use the better fluid for the patient.
Other drugs in Crystalloids
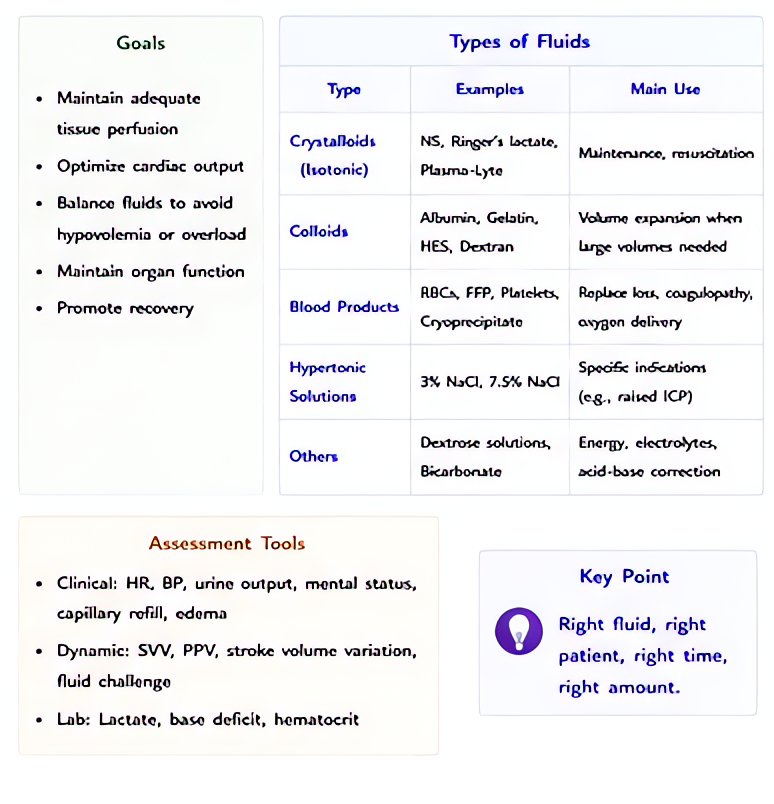
- Lactated Ringer's (LR / Hartmann's solution)
Na⁺ 130, Cl⁻ 109, K⁺ 4, Ca²⁺ 3, lactate 28 mEq/L; osmolality 273 mOsm/kg (slightly hypotonic). Lactate metabolized by liver to bicarbonate, providing buffering. Closer to plasma electrolyte composition than saline.
- Plasma-Lyte 148 (and similar balanced solutions)
Na⁺ 140, Cl⁻ 98, K⁺ 5, Mg²⁺ 3, acetate 27, gluconate 23 mEq/L; osmolality 294 mOsm/kg. Acetate and gluconate metabolize independent of liver perfusion (unlike lactate), making it useful in liver failure / shock states. No calcium → fully compatible with blood products.
- D5W (5% Dextrose in Water)
5% dextrose (50 g/L) in water — when dextrose is metabolized, the remaining solution is free water. Effectively a free-water source distributed across total body water (28–42 L in adult).
- Hypertonic Saline 3% (and 23.4%)
3% NaCl: Na⁺ 513 mEq/L, osmolality 1027 mOsm/kg. 23.4% NaCl: Na⁺ 4000 mEq/L. Pulls water from brain parenchyma across an intact blood-brain barrier into the intravascular space — reduces ICP and treats severe hyponatremia.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e