Hypertonic Saline 3% (and 23.4%)
3% NaCl · 23.4% NaCl
Hypertonic crystalloid (osmotherapy)
3% NaCl: Na⁺ 513 mEq/L, osmolality 1027 mOsm/kg. 23.4% NaCl: Na⁺ 4000 mEq/L. Pulls water from brain parenchyma across an intact blood-brain barrier into the intravascular space — reduces ICP and treats severe hyponatremia.
Indications
- •Acute symptomatic hyponatremia (seizure, coma) — 100 mL bolus 3% NaCl, repeat × 2 if needed
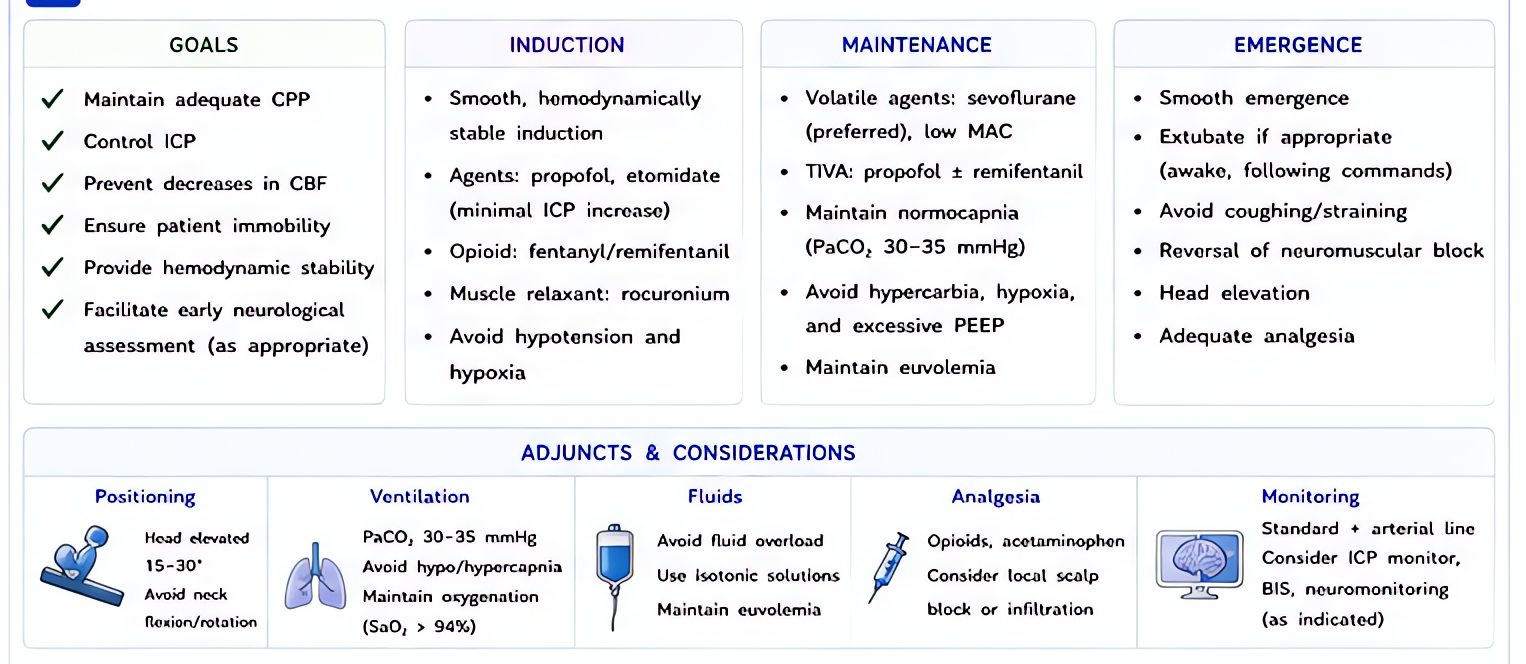
- •Elevated intracranial pressure (TBI, intracranial mass with herniation, ICH)
- •Cerebral salt wasting / SIADH refractory to fluid restriction
- •Hyponatremia in cirrhosis with neurologic symptoms
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Symptomatic hyponatremia (seizure/coma) | 100 mL 3% NaCl IV over 10 min; repeat × 2 if symptoms persist; target Na rise 4–6 mEq/L in first 6 h, ≤10 mEq/L in 24 h | — |
| Elevated ICP, ongoing | 3% infusion 30–100 mL/h titrated to Na 145–155 mEq/L and osm 300–320 mOsm/kg | — |
| Acute herniation rescue | 23.4% NaCl 30 mL central line over 5–10 min; OR 3% NaCl 250–500 mL over 30 min | — |
Pharmacokinetics
Onset minutes for ICP reduction. Effect lasts 4–6 h; sustained with infusion.
Hemodynamic effects
Transient volume expansion + transient ↑BP from osmotic effect. Useful in hypotensive TBI patient where mannitol's diuresis would worsen hypotension.
Respiratory effects
Pulmonary edema in cardiac patients (volume + sodium load).
Side effects
- !Osmotic demyelination syndrome (central pontine myelinolysis) if Na corrected too rapidly (>10 mEq/L in 24 h)
- !Hyperchloremic metabolic acidosis at sustained doses
- !Hypernatremia at planned osmotherapy targets
- !Acute kidney injury at osm >320 mOsm/kg
- !Pulmonary edema in cardiac patients
- !Phlebitis — peripheral 3% NaCl irritates veins; central line preferred for sustained infusion
- !Local tissue necrosis from extravasation (especially 23.4%)
Contraindications
- ×Hypernatremia (>155 mEq/L) without need for osmotherapy
- ×Severe CHF without ICP / hyponatremia indication
- ×Inability to monitor Na levels q4–6 h
Clinical pearls
- ★PREFERRED OVER MANNITOL IN HYPOTENSIVE TBI: hypertonic saline expands volume + reduces ICP simultaneously; mannitol diureses and can worsen hypotension. SCCM/ENLS guidelines call hypertonic saline first-line for elevated ICP in patients with hemodynamic instability.
- ★OSMOTIC DEMYELINATION: most feared complication. Risk factors = chronic hyponatremia (>48 h), alcoholism, malnutrition, hypokalemia, liver disease. RATE LIMIT: Na rise ≤10 mEq/L per 24 h, ≤18 mEq/L per 48 h. If you overshoot, reverse with D5W and DDAVP — multiple case reports of successful re-lowering.
- ★23.4% IS A CENTRAL-LINE-ONLY PRODUCT (rare exception via large peripheral in genuine herniation rescue with no central access). Extravasation of 23.4% causes severe tissue necrosis.
- ★100 mL × 3 RULE FOR SYMPTOMATIC HYPONATREMIA: 100 mL of 3% NaCl raises Na ~2–3 mEq/L. Three boluses over 60 min raise Na 6–9 mEq/L — typically resolves seizures.
- ★DISRUPTED BBB: unlike mannitol (which can worsen edema with disrupted BBB), hypertonic saline remains effective when BBB is impaired — reason it's preferred in penetrating TBI and complex craniotomy.
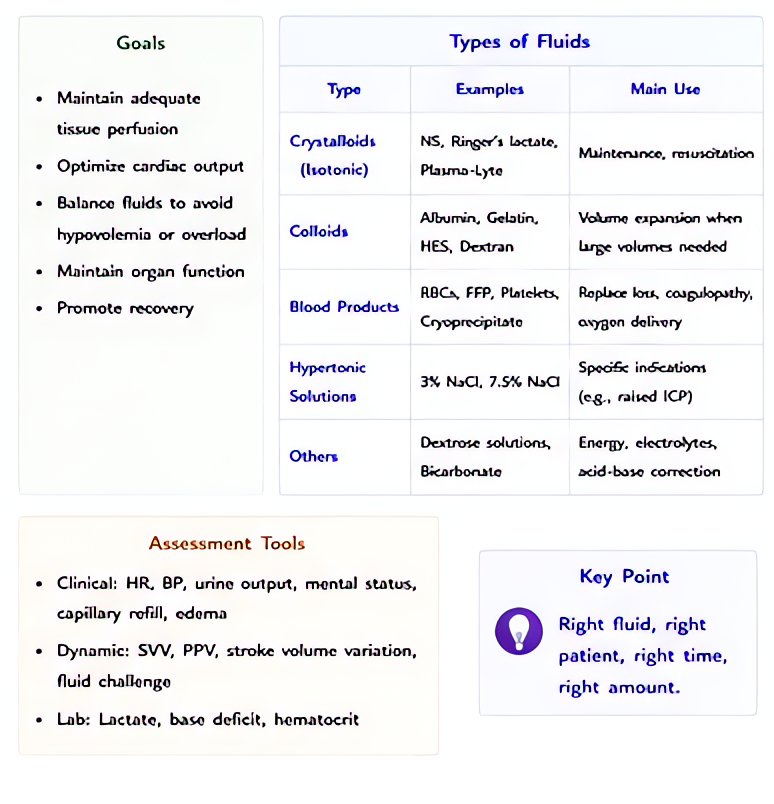
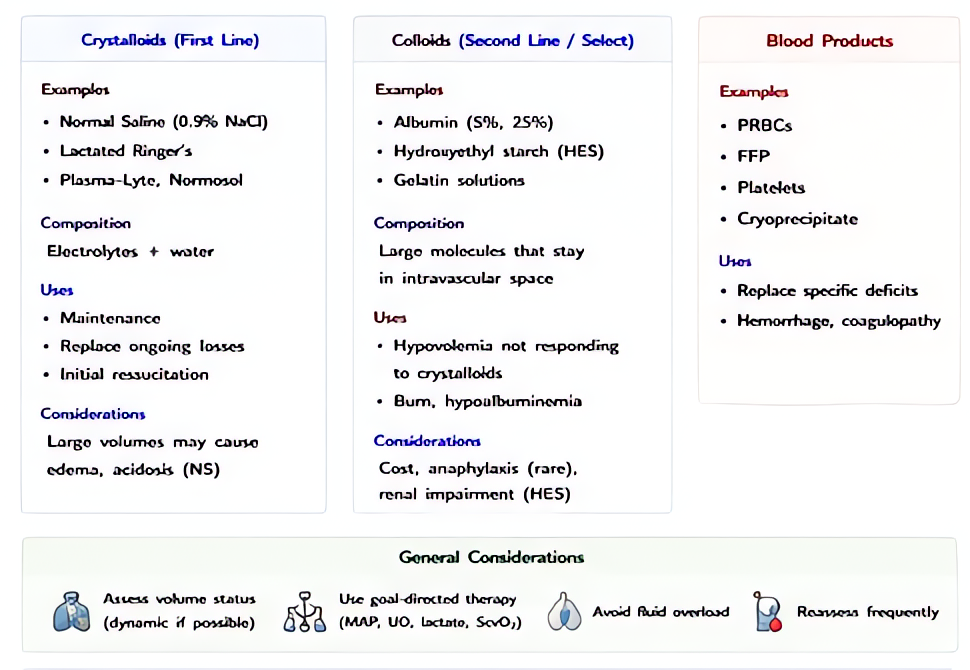
Other drugs in Crystalloids
- Normal Saline (0.9% NaCl)
0.9% sodium chloride in water — Na⁺ 154 mEq/L, Cl⁻ 154 mEq/L, osmolality 308 mOsm/kg. Distributes throughout the extracellular space; ~25–30% of infused volume remains intravascular at 30–60 min.
- Lactated Ringer's (LR / Hartmann's solution)
Na⁺ 130, Cl⁻ 109, K⁺ 4, Ca²⁺ 3, lactate 28 mEq/L; osmolality 273 mOsm/kg (slightly hypotonic). Lactate metabolized by liver to bicarbonate, providing buffering. Closer to plasma electrolyte composition than saline.
- Plasma-Lyte 148 (and similar balanced solutions)
Na⁺ 140, Cl⁻ 98, K⁺ 5, Mg²⁺ 3, acetate 27, gluconate 23 mEq/L; osmolality 294 mOsm/kg. Acetate and gluconate metabolize independent of liver perfusion (unlike lactate), making it useful in liver failure / shock states. No calcium → fully compatible with blood products.
- D5W (5% Dextrose in Water)
5% dextrose (50 g/L) in water — when dextrose is metabolized, the remaining solution is free water. Effectively a free-water source distributed across total body water (28–42 L in adult).
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e