Venous Air Embolism (VAE) — Sitting Craniotomy
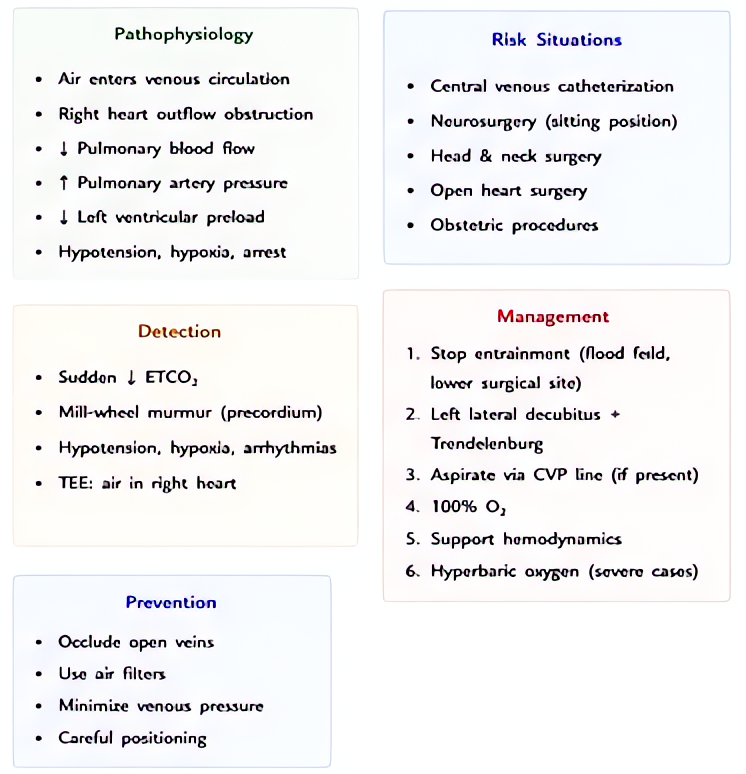
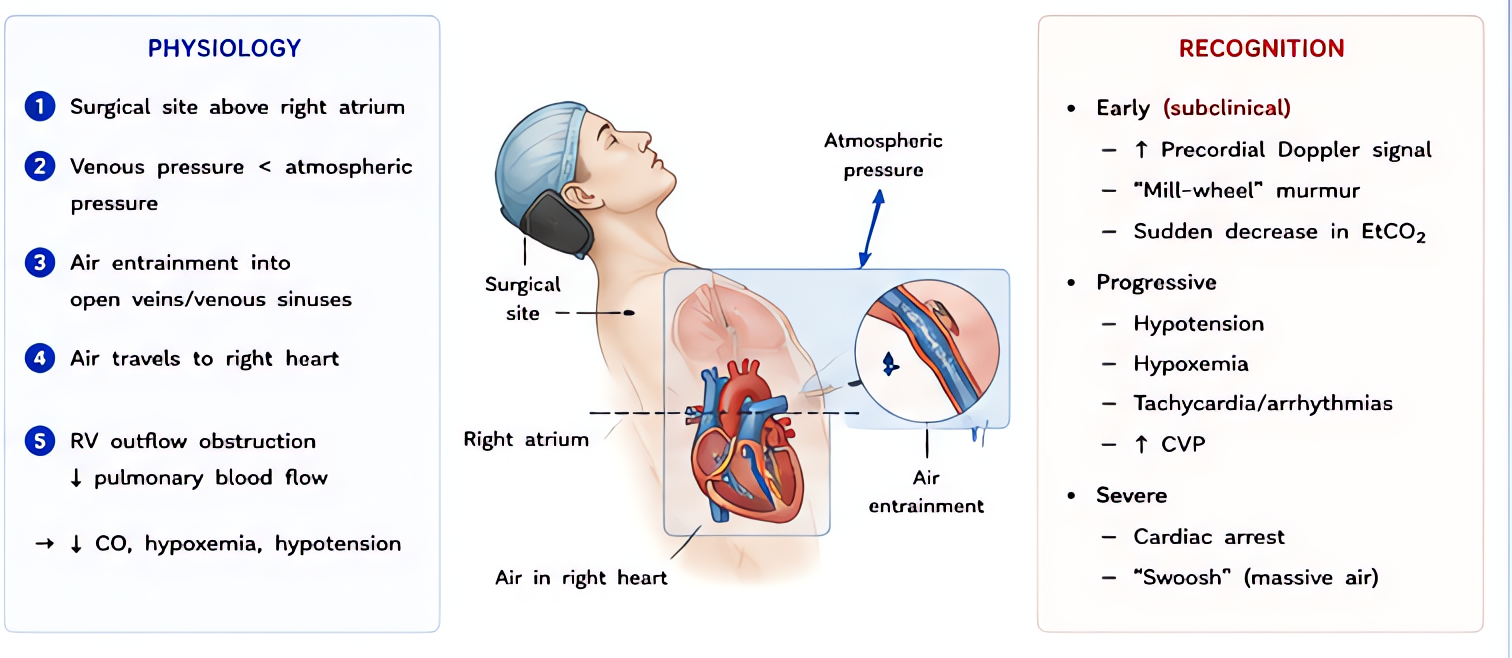
Air entry through open venous sinuses with patient above heart. Sudden ↓ ETCO2, hypoxemia, hypotension, mill-wheel murmur. Notify surgeon, flood field, support hemodynamics, aspirate via PAC or central line.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •Sudden ↓ ETCO2 (sensitive, early)
- •Doppler precordial chirp / mill-wheel murmur (not always heard)
- •Hypotension + arrhythmia + hypoxemia
- •Setting: sitting craniotomy, posterior fossa, cervical spine surgery, CVC insertion, laparoscopy
- •TEE most sensitive — bubbles in right heart
Steps
- 1Notify surgeon immediately — flood surgical field with saline, pack with wet gauze
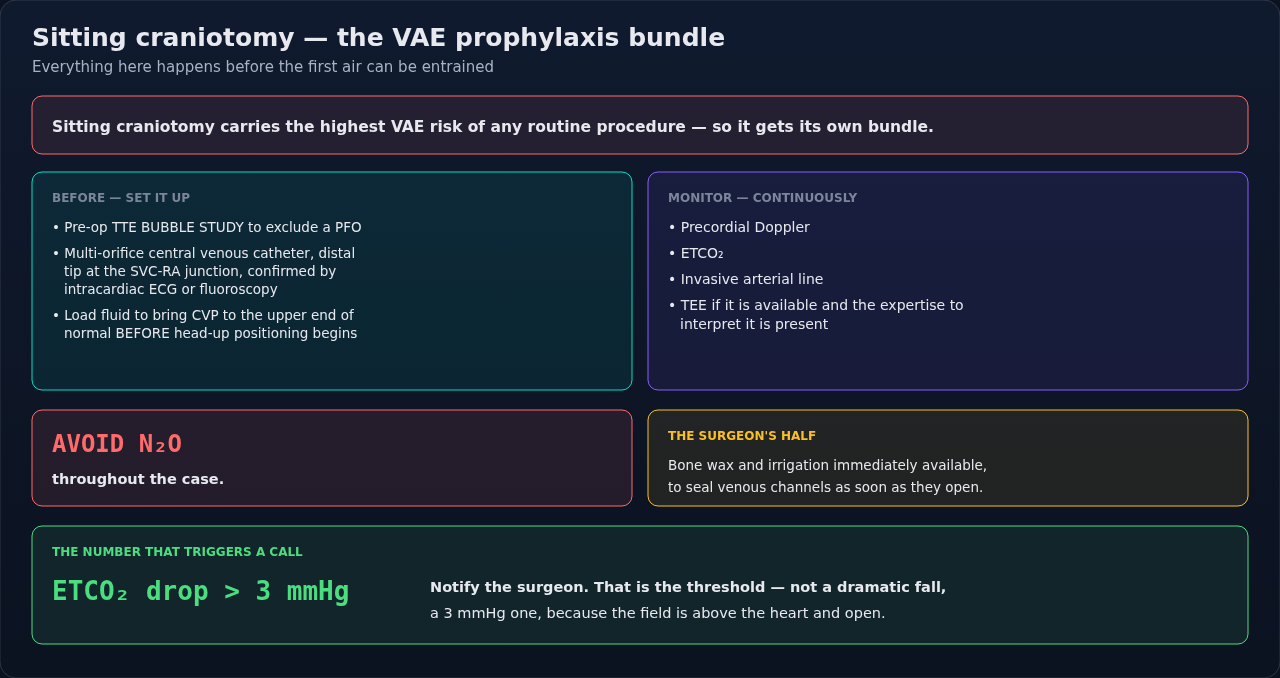
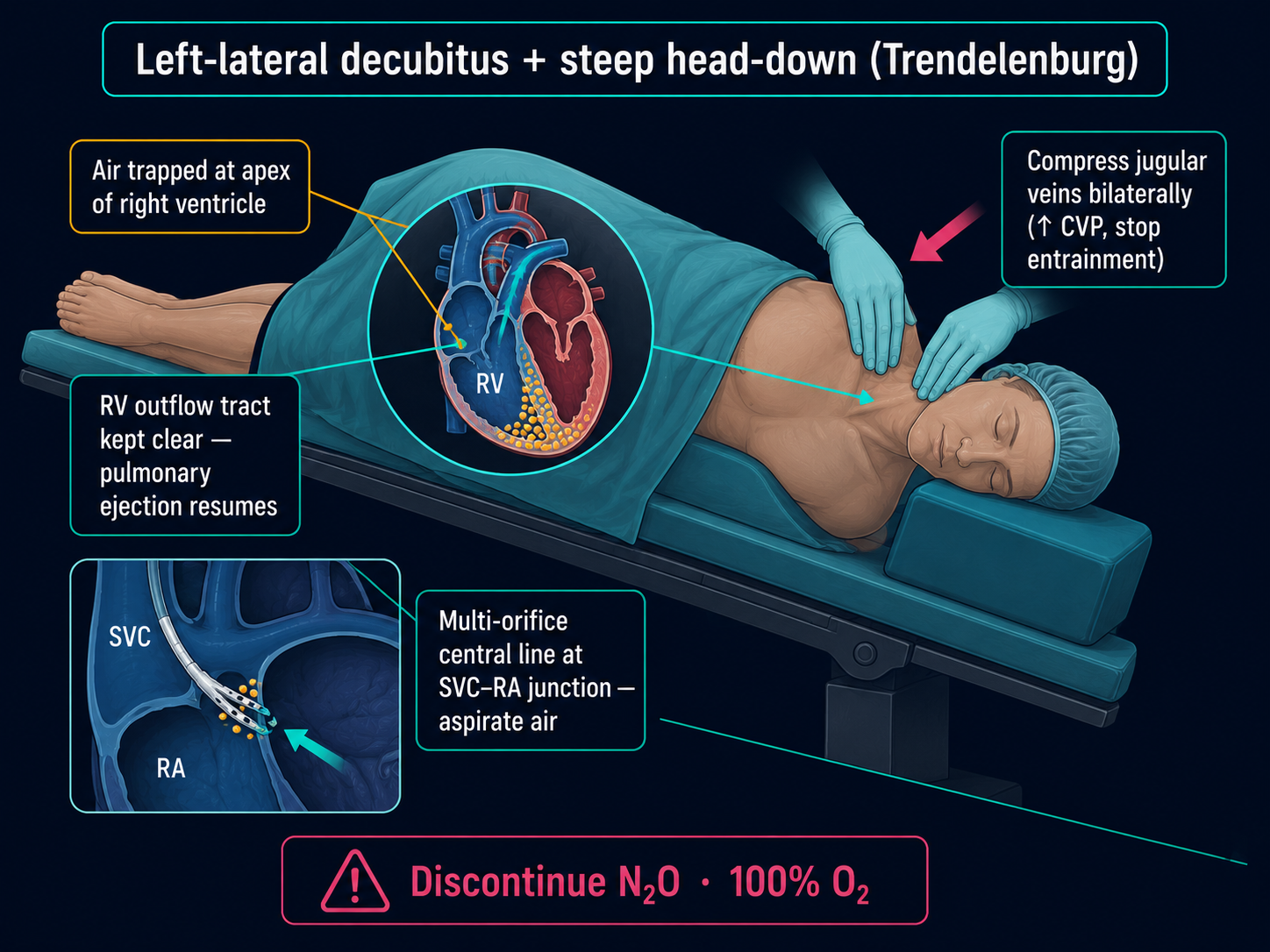
- 2100% FiO2 + discontinue N2O if runningN2O expands air emboli — never use in cases at risk.
- 3Compress jugular veins (bilateral) — increases venous pressure at surgical site, prevents further entrainment
- 4Position — left lateral decubitus + head down (Durant maneuver)Traps air in right atrium apex, away from RVOT.
- 5Aspirate air via central line / PAC if available — multi-orifice CVC at SVC-RA junction is ideal
- 6Hemodynamic support — vasopressors, fluids, treat right heart strain
- 7If cardiac arrest: ACLS + lateral decubitus + aggressive aspiration + consider ECMO
- 8Post-event: ICU monitoring, paradoxical embolism check (echo + neuro exam if PFO suspected)
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Norepinephrine | 0.05-0.5 mcg/kg/min infusion | |
| Phenylephrine | 100-200 mcg IV bolus | |
| Epinephrine | 10-100 mcg IV bolus if cardiac arrest imminent |
Pitfalls
- !NEVER use N2O in sitting craniotomy or cases with VAE risk — N2O expands air bubbles.
- !Precordial Doppler is the most sensitive non-TEE monitor — listen at 2nd-3rd ICS right sternal border.
- !Paradoxical embolism through PFO → stroke — image post-event if any neuro deficit.
- !Sitting position requires pre-induction echo to rule out PFO in many institutions.
Suggested reading
- Mirski et al. Anesthesiology 2007
- Miller's 9e Ch 70 (Neuro Anesthesia)
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.