Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
⚡ Rehearsal mode
Walk the algorithm step by step
7 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •Inspiratory stridor (partial) → silent chest with paradoxical movement (complete)
- •Rising PIP with no CO₂ trace
- •Desaturation despite bagging
- •Common during light anesthesia: induction, emergence, secretions
Steps
- 1100% FiO₂, remove noxious stimulusStop suctioning, surgical stim; suction blood/secretions away from cords.
- 2Larson's maneuver + jaw thrustBilateral firm pressure at the styloid notch (behind the earlobe). Often breaks the spasm.
- 3CPAP 15–20 cm H₂O with tight mask seal
- 4Deepen anesthesiaPropofol 0.5–1 mg/kg IV breaks light-plane spasm.
- 5Succinylcholine 0.1–0.5 mg/kg IV (or 4 mg/kg IM if no IV)CONTENT-AUDIT #1 (2026-06-10): IM dose corrected to 4 mg/kg single-dose (per Miller's 9e + Coté Pediatric Anesthesia 7e); prior range 2–4 mg/kg underdosed for reliable rapid laryngospasm relief. IM works through the deltoid in 60–90 sec; vastus lateralis is also acceptable in peds.
- 6Atropine 0.02 mg/kg IV in pediatricsPrevents reflex bradycardia from sux + hypoxia.
- 7Re-intubate + suction + secure if recurrent
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Propofol | 0.5–1 mg/kg IV | |
| Succinylcholine | 0.1–0.5 mg/kg IV; 4 mg/kg IM | |
| Atropine | 0.02 mg/kg IV (peds; min 0.1 mg) |
Pitfalls
- !Forced positive pressure with poor seal pushes O₂ into the stomach, not lungs.
- !Do NOT give sux to a cold induction in suspected MH-susceptible patient.
- !Re-extubate deep, not light, in patients with reactive airways.
Suggested reading
- AANA Practice Considerations: Airway
- Hampson-Evans Paediatr Anaesth 2008
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.
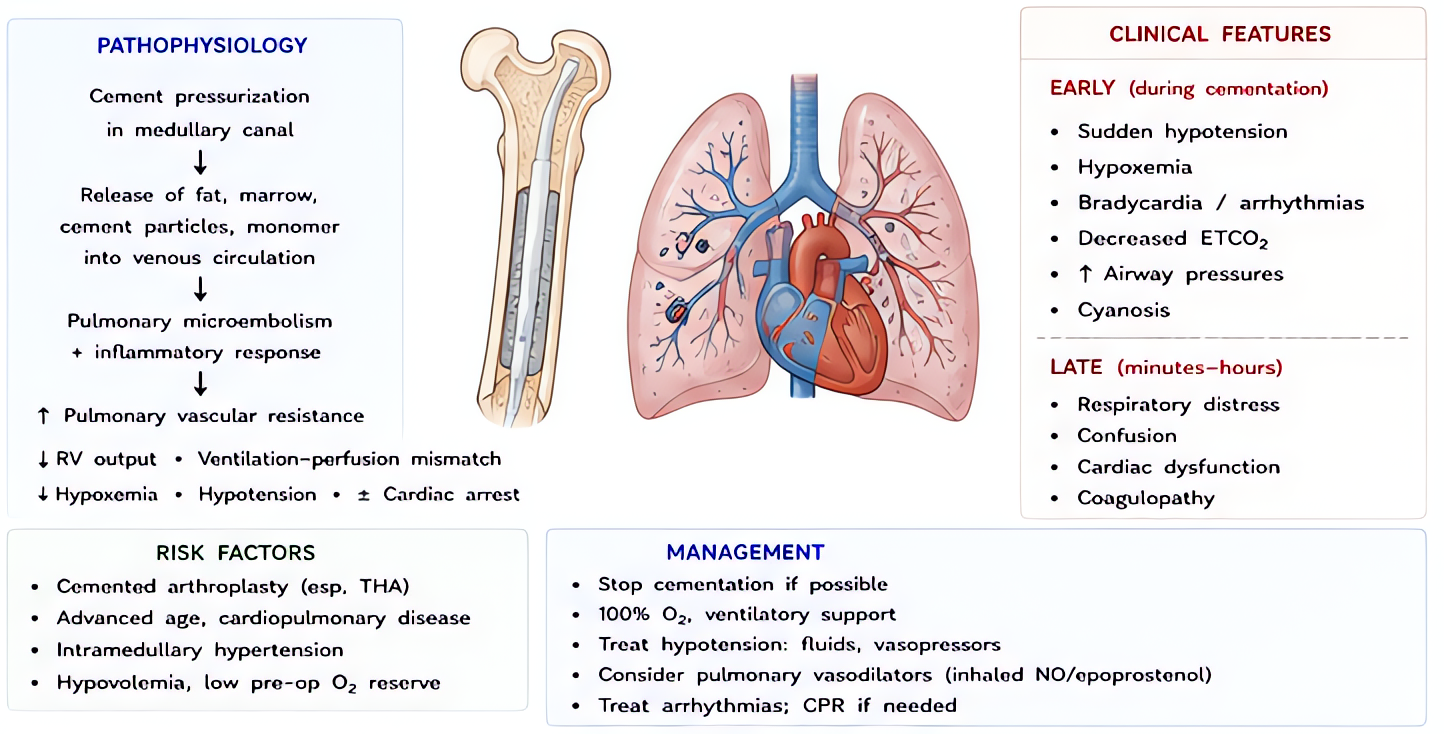
- Intraoperative Pulmonary Embolism
Sudden ↑PA pressure → RV failure → cardiovascular collapse. May be thrombus, fat (long-bone fracture, IM rod), gas (laparoscopy CO₂, sitting craniotomy), or amniotic.