Severe Bronchospasm / Status Asthmaticus in OR
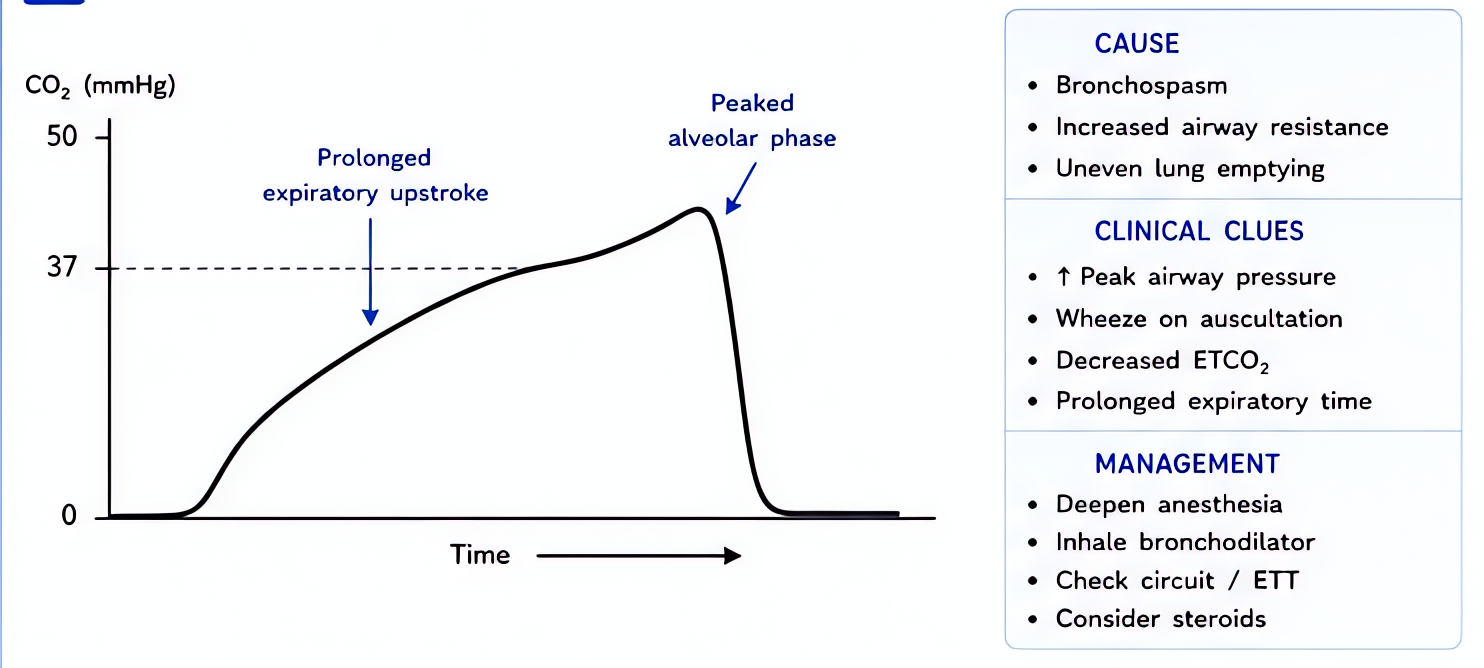
Sudden ↑ peak airway pressure + wheezing + ↑ ETCO2 plateau slope. Treat by deepening anesthesia (volatile bronchodilation), beta-2 agonist, and adjuncts. Avoid agents that worsen bronchospasm.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
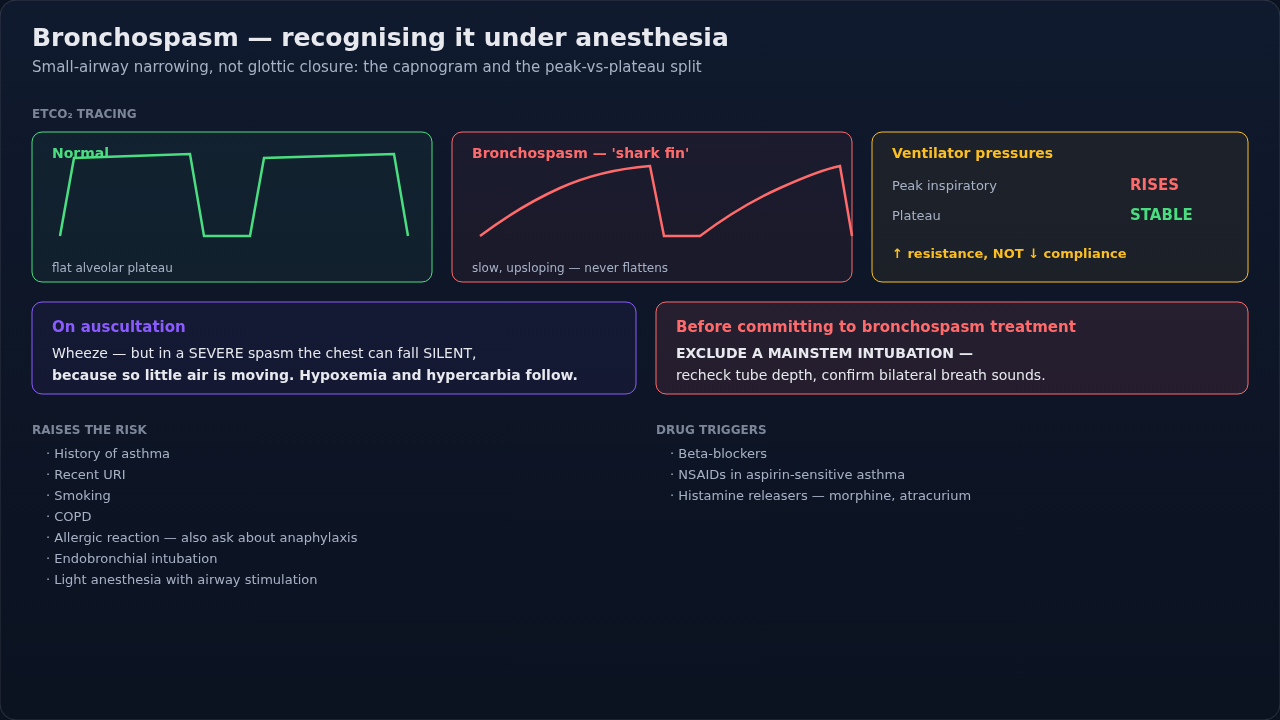
Recognition
- •Sudden ↑ peak inspiratory pressure (>40 cmH2O typical)
- •Wheezing on auscultation; expiration prolonged
- •Capnogram: shark-fin pattern (upsloping plateau)
- •Falling SpO2 + rising ETCO2 if obstruction severe
- •Setting: known asthma + light anesthesia + airway stimulation
Steps
- 1Increase FiO2 to 1.0 + manual ventilation to assess compliance
- 2Deepen anesthesia — volatile (sevoflurane preferred) is potent bronchodilatorIso/sevo/des all bronchodilate. Avoid des if naive (airway irritation).
- 3Albuterol via ETT — 8-10 puffs into the circuitMDI adapter or nebulizer. Most goes to circuit walls — overdose intentionally.
- 4IV epinephrine if refractory or hypotension10-100 mcg bolus, infusion 0.05-0.5 mcg/kg/min.
- 5Magnesium sulfate 2g IV over 20 min
- 6Ketamine — 0.5-1 mg/kg IV bolus or 0.5-1 mg/kg/hr infusionBronchodilator + maintains anesthesia.
- 7Steroids (slow onset but adjunct)Methylpred 125 mg or hydrocortisone 100 mg IV.
- 8Allow longer expiration — extend I:E to 1:3 or 1:4; risk auto-PEEPDisconnect ETT if breath stacking → exhale → reconnect.
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Albuterol MDI | 8-10 puffs in-circuit, q15 min | |
| Epinephrine | 10-100 mcg IV bolus; infusion 0.05-0.5 mcg/kg/min | |
| Magnesium sulfate | 2g IV over 20 min | |
| Ketamine | 0.5-1 mg/kg IV bolus | |
| Methylprednisolone | 125 mg IV (anti-inflammatory; slow onset) | |
| Sevoflurane | Titrate to 1.5-2 MAC for deep anesthesia |
Pitfalls
- !AVOID histamine-releasing agents (atracurium, morphine) in severe asthma.
- !Beta-blockers contraindicated in severe bronchospasm.
- !Auto-PEEP from incomplete exhalation — disconnect to allow full exhalation.
- !Don't extubate in deep anesthesia in severe asthma → laryngospasm trigger; wake fully.
Suggested reading
- GINA Guidelines 2024
- Miller's 9e Ch 53
- AANA Anesthesia in Asthma Position
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.