Refractory / Catecholamine-Resistant Hypotension
BP fails to respond to escalating norepinephrine + fluids. Consider vasopressin, methylene blue, hydroxocobalamin, hydrocortisone, and specific etiology (anaphylaxis, vasoplegia, ACEi-related, sepsis, addisonian).
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •MAP <65 despite NE >0.5 mcg/kg/min + adequate volume
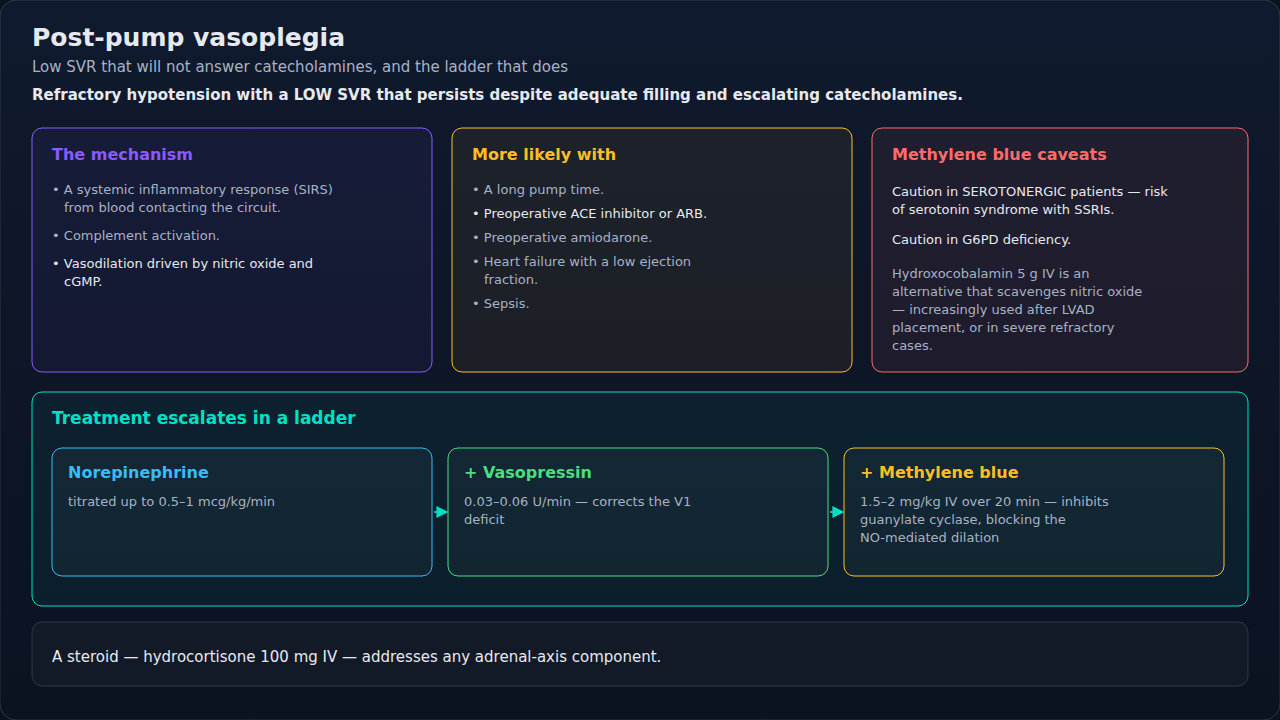
- •After CPB — vasoplegic syndrome (low SVR, normal CO)
- •Septic shock with high lactate + maximal NE
- •ACEi/ARB taken pre-op + persistent hypotension despite vasopressors
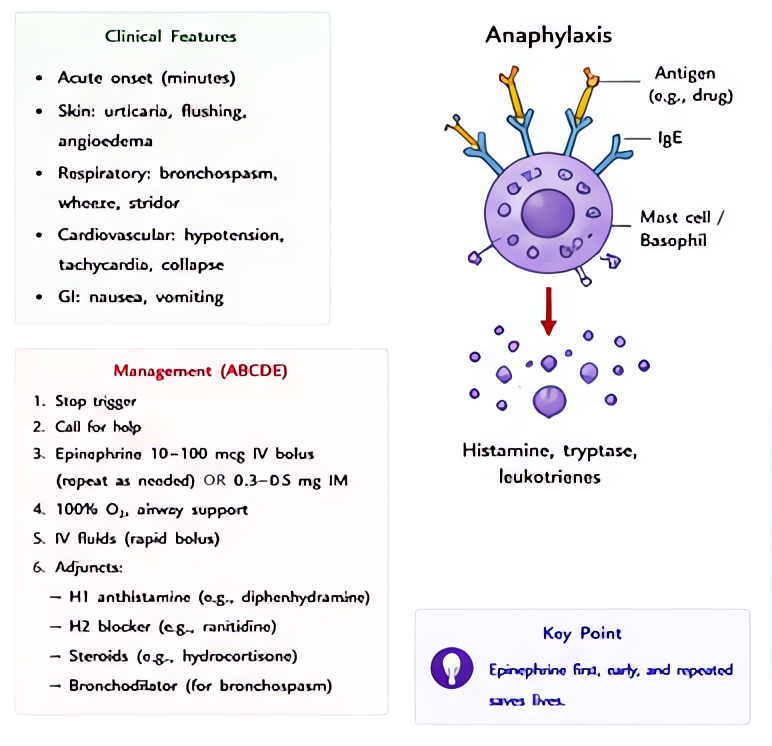
- •Anaphylaxis refractory to epinephrine (consider methylene blue)
Steps
- 1Re-assess and confirm — A-line accurate? Volume actually adequate? Cardiac function (TEE/echo)?
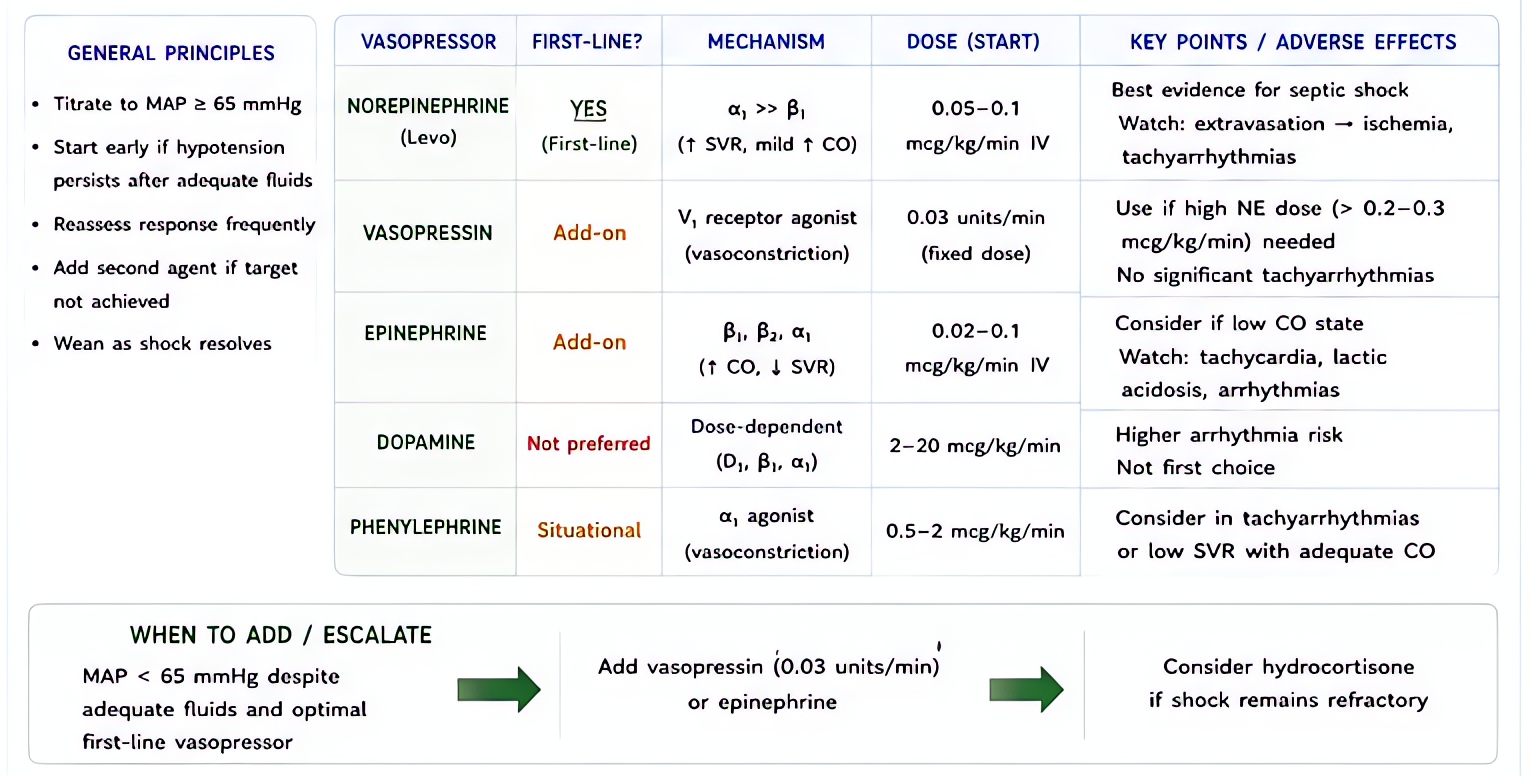
- 2Add second-line vasopressor: vasopressin 0.03-0.04 U/min infusionActs via V1 receptors — bypasses adrenergic pathway. Especially useful in sepsis + vasoplegia.
- 3Hydrocortisone 100 mg IV q8h if relative adrenal insufficiency suspectedEspecially refractory septic shock + chronic steroid use.
- 4Methylene blue 1-2 mg/kg IV bolus over 20 minNO synthase inhibitor — reverses NO-mediated vasodilation. Refractory anaphylaxis, post-CPB vasoplegia, anaphylactoid.
- 5Hydroxocobalamin 5g IV (Cyanokit)NO scavenger — for refractory vasoplegia post-CPB or post-LVAD.
- 6Calcium chloride 1g IV — esp if citrate load (massive transfusion) or post-CPB
- 7Mechanical support — if cardiogenic component: IABP, Impella, ECMO
- 8Treat etiology — anaphylaxis (epi), sepsis (source control), bleeding (transfuse), tamponade (drain)
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Vasopressin | 0.03-0.04 U/min infusion (no titration window — fixed dose) | |
| Methylene blue | 1-2 mg/kg IV over 20 min; may repeat ×1 | |
| Hydroxocobalamin (Cyanokit) | 5g IV over 15 min | |
| Hydrocortisone | 100 mg IV q8h | |
| Calcium chloride | 1g IV bolus | |
| Angiotensin II (Giapreza) | 10 ng/kg/min IV titrate (high-output shock) |
Pitfalls
- !Methylene blue contraindicated in G6PD deficiency (causes hemolysis) + serotonin syndrome with SSRIs/MAOIs.
- !Don't escalate norepinephrine indefinitely — switch class once at 0.5 mcg/kg/min.
- !Echo first — pure pump failure needs inotropy not vasoconstriction.
- !ACEi-related hypotension: vasopressin works when phenylephrine + NE fail.
Suggested reading
- Surviving Sepsis 2021
- ATHOS-3 Trial NEJM 2017
- Miller's 9e Ch 102
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.