Severe Pre-eclampsia / Eclampsia / HELLP
Pregnancy-induced hypertension + end-organ dysfunction. Mag for seizure prophylaxis, BP control to 140-160/90-110, deliver if severe features. Eclampsia = seizure → mag + airway + delivery.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
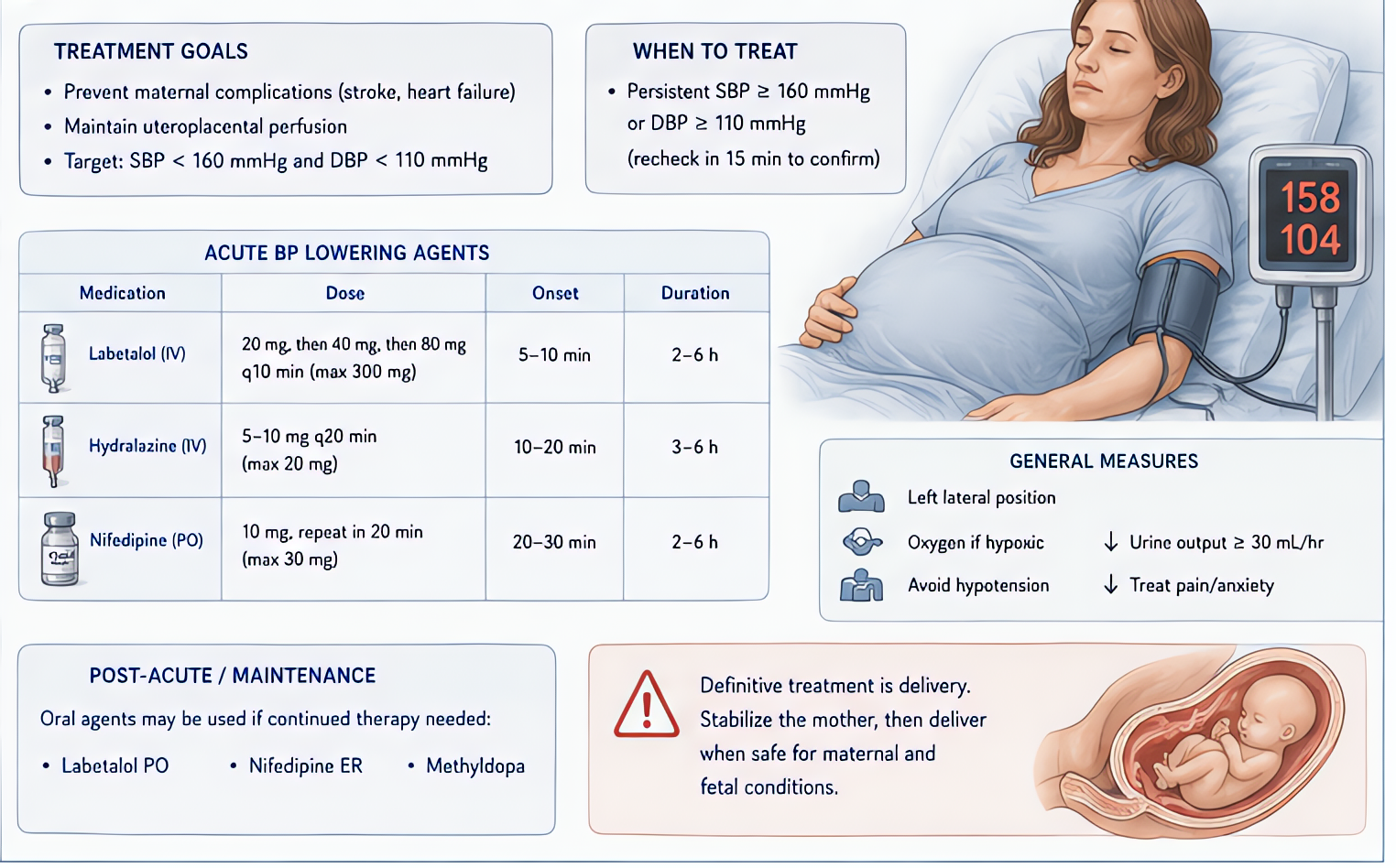
- •Severe pre-eclampsia: BP ≥160/110, headache, visual changes, RUQ pain, proteinuria >5g/24h, oliguria, plt <100k, transaminitis, pulmonary edema
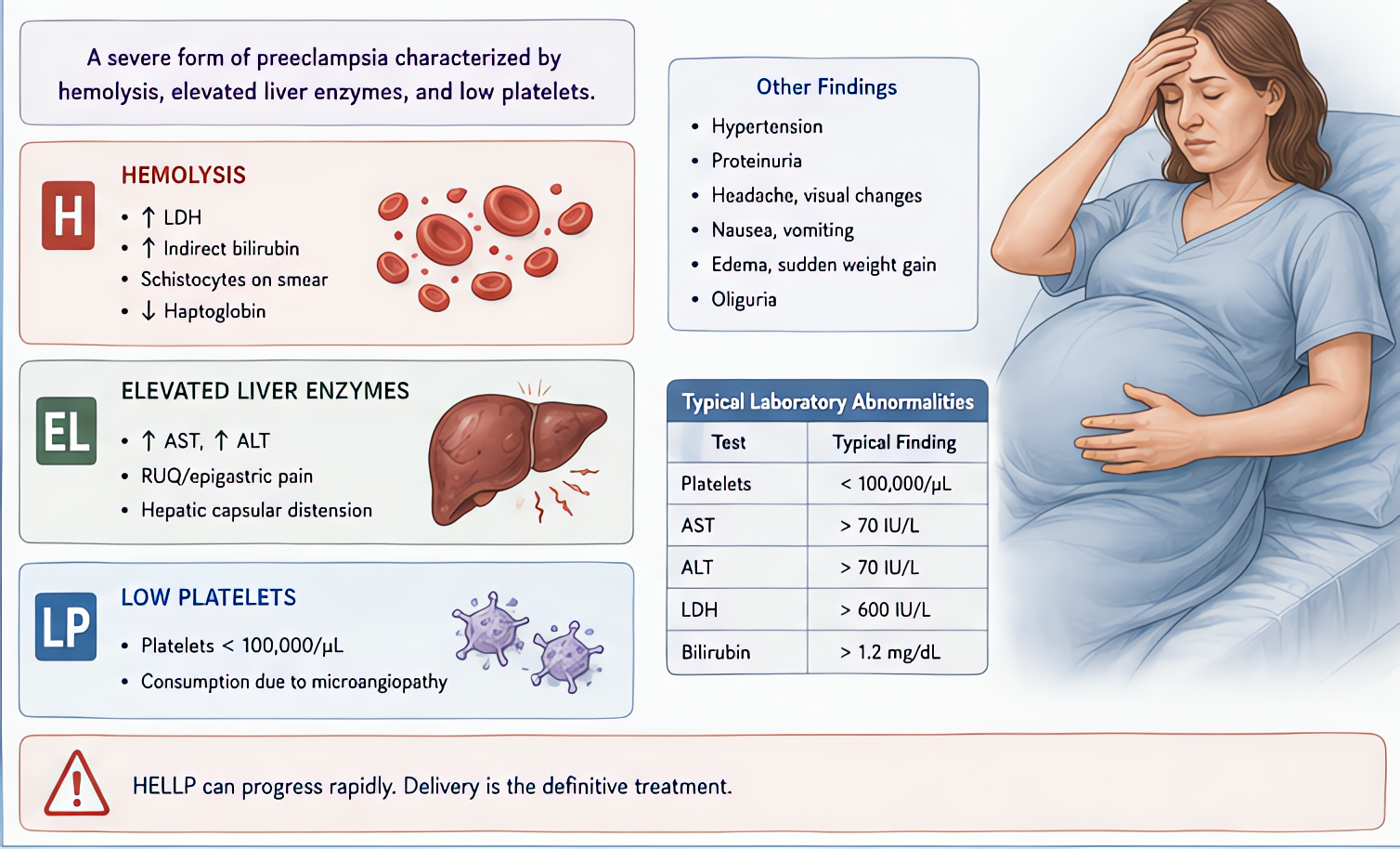
- •HELLP: Hemolysis (LDH ↑, schistocytes), Elevated Liver enzymes, Low Platelets
- •Eclampsia: tonic-clonic seizure in pregnancy or postpartum
- •Atypical eclampsia possible without HTN/proteinuria
Steps
- 1Position lateral decubitus + secure airway + 100% O2 + IV access
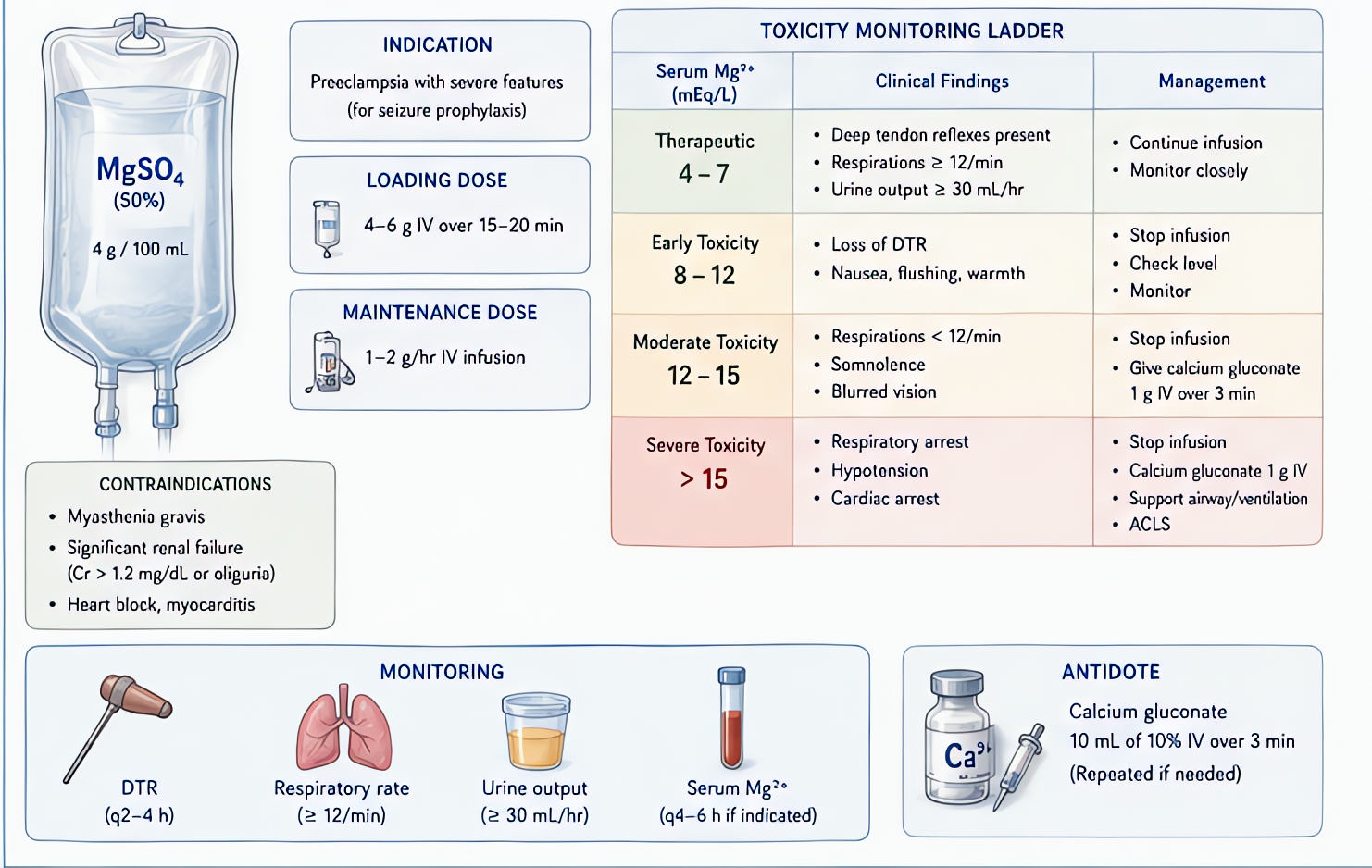
- 2Magnesium sulfate — 4-6g IV load over 20 min, then 1-2g/hr infusionContinue until 24h post-delivery or 24h post-last-seizure. Monitor reflexes (DTRs lost at 8-10 mEq/L), respiratory rate.
- 3Antihypertensive — labetalol 10-20 mg IV q10 min OR hydralazine 5-10 mg IV q20 min OR nicardipine infusionGoal BP 140-160 / 90-110. AVOID over-correction (placental hypoperfusion).
- 4Eclampsia: mag bolus 4-6g IV; if persistent — additional 2g; benzodiazepine if mag fails
- 5Assess fetal status (continuous FHR monitoring)
- 6Plan delivery — if ≥34 wks deliver immediately; <34 wks consider maternal/fetal balance
- 7Anesthesia for CS: neuraxial preferred if plt ≥70-100k + no bleeding diathesisGA if airway concerns, severe coagulopathy, or rapid delivery needed.
- 8Mag toxicity (lost DTRs, RR <12, weakness) — STOP infusion, give calcium gluconate 1g IV
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Magnesium sulfate | 4-6g IV load over 20 min, 1-2g/hr infusion | |
| Labetalol | 10-20 mg IV, double q10 min, max 220 mg | |
| Hydralazine | 5-10 mg IV q20 min | |
| Nicardipine | 5-15 mg/hr IV infusion | |
| Calcium gluconate | 1g IV over 10 min — for mag toxicity |
Pitfalls
- !AVOID nifedipine + magnesium together — synergistic hypotension + neuromuscular blockade.
- !Ergots (methylergonovine) contraindicated in pre-eclampsia for PPH — use other uterotonics.
- !Plt count + coag at induction — neuraxial OK if plt ≥70k stable + no antiplatelet/antico.
- !Don't treat BP too aggressively — placental hypoperfusion + fetal distress.
- !Mag potentiates non-depolarizing NMB — reduce dose by 50%.
Suggested reading
- ACOG Hypertension in Pregnancy Bulletin
- Magpie Trial Lancet 2002
- Chestnut OB Anesthesia 6e
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.