PALS — Pediatric Cardiac Arrest
Pediatric arrest is most often respiratory in origin. Highest-quality CPR + addressing airway/breathing precedes rhythm management. Asystole/PEA is the most common arrest rhythm in children.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •Unresponsive + no normal breathing + no central pulse within 10 sec
- •Bradycardia <60/min with poor perfusion = start CPR (peds-specific)
- •Most pediatric arrest = hypoxic/asphyxial; address airway/breathing first
Steps
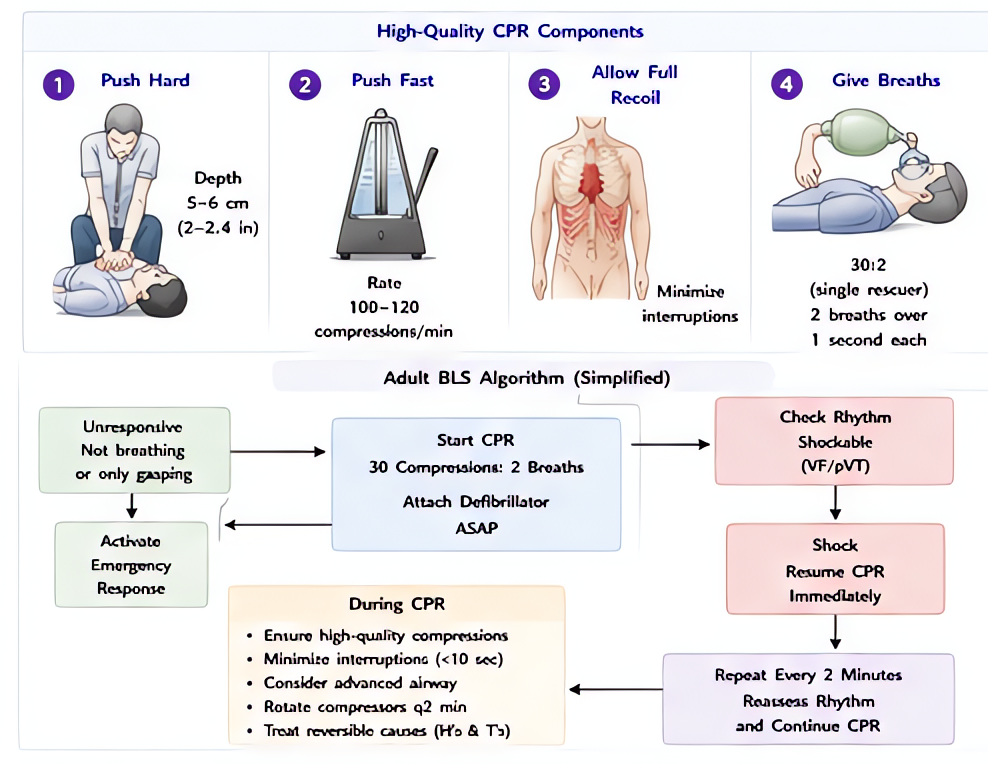
- 1Start CPR — 30:2 (single rescuer) or 15:2 (two rescuers, peds)Rate 100-120/min; depth ~1/3 AP chest (~1.5 in infant, ~2 in child).
- 2Attach defib pads + assess rhythm at 2-min cycle
- 3If shockable (VF/pVT) — defib 2 J/kg; subsequent 4 J/kg (max 10 J/kg or adult)
- 4If non-shockable (asystole/PEA) — continue CPR + epinephrine
- 5Epinephrine 0.01 mg/kg IV/IO q3-5 minMax 1 mg single dose. Give ASAP in non-shockable rhythms.
- 6Identify + treat reversible causes (H's & T's)Hypoxia + hypovolemia top of list in peds.
- 7Advanced airway when feasible — ETT or supraglotticContinuous compressions once advanced airway placed; ventilate 1 q2-3 sec.
- 8Post-ROSC: targeted temperature management — AHA/PALS 2020 + THAPCA accepts EITHER 32–34°C OR 36–37.5°C × 5 days continuous monitoring; avoid hyperoxia + hyperthermia
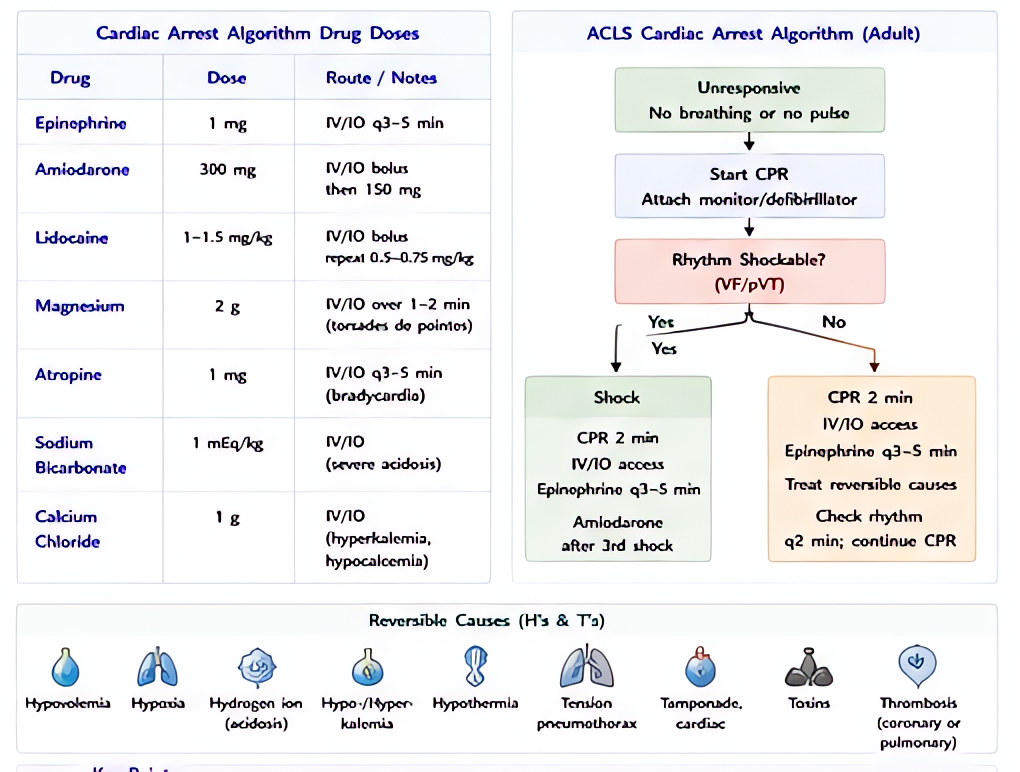
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Epinephrine | 0.01 mg/kg IV/IO (0.1 mL/kg of 1:10,000) | |
| Amiodarone | 5 mg/kg IV/IO bolus (refractory VF/pVT, may repeat ×2) | |
| Lidocaine | 1 mg/kg IV/IO (alternative to amiodarone) | |
| Magnesium sulfate | 25-50 mg/kg IV/IO for torsades (max 2g) | |
| Atropine | 0.02 mg/kg (min 0.1 mg) for bradycardia from primary AV block |
Pitfalls
- !Do NOT use a defib energy >10 J/kg even if adult dose is lower.
- !Bradycardia <60 with poor perfusion = CPR; do not wait for asystole.
- !Avoid hyperventilation post-ROSC — worsens cerebral perfusion.
- !Length-based tape (Broselow) for weight estimation if unknown.
Suggested reading
- AHA PALS 2020
- Coté Pediatric Anesthesia 7e
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.