Obstetric Hemorrhage (PPH / Atony / Placenta)
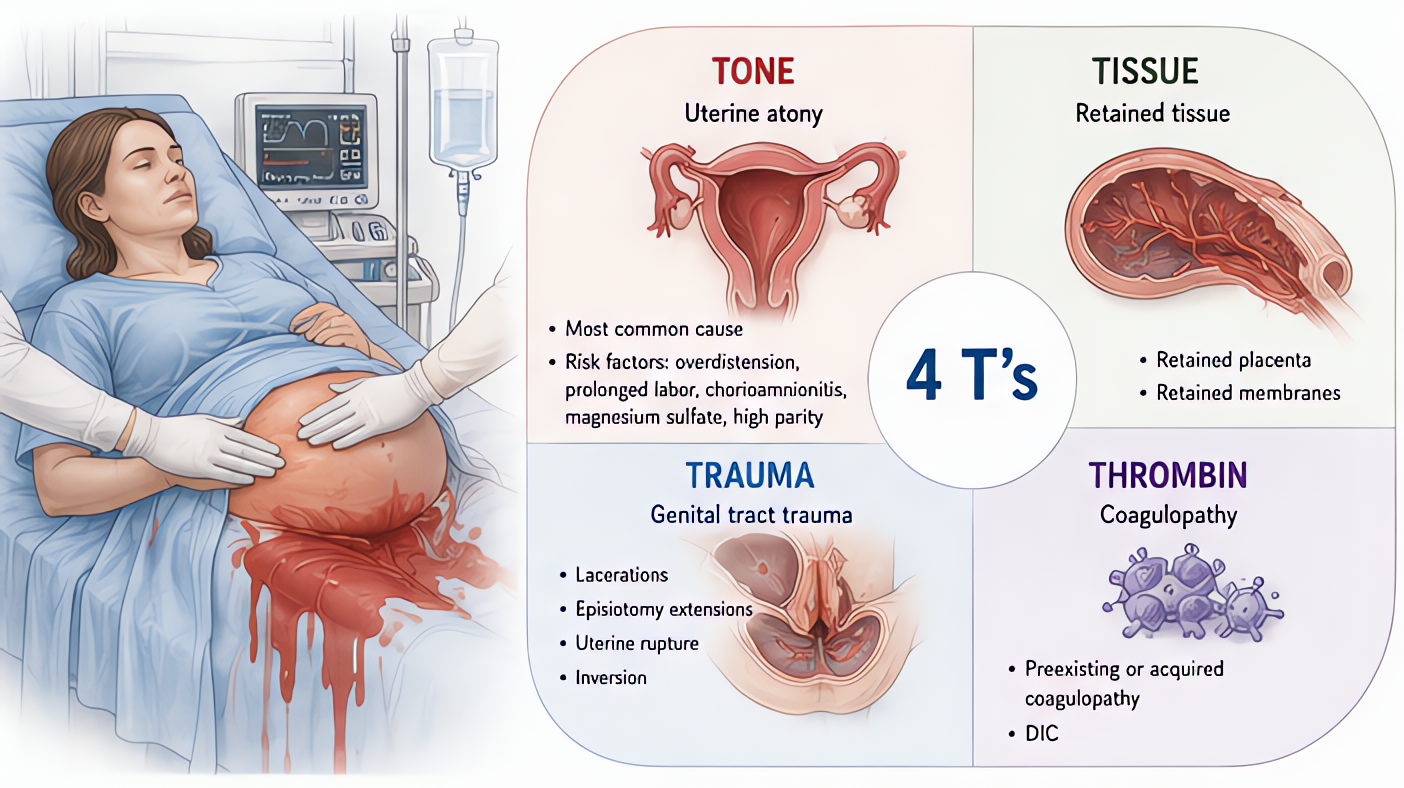
Most common cause of maternal mortality worldwide. 4 T's: Tone (atony 70%), Trauma (laceration), Tissue (retained placenta), Thrombin (coagulopathy). Stage-based response: massage → uterotonics → balloon → surgical.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •Stage 1: 500-1000 mL EBL post-vaginal or 1000+ mL post-CS without abnormal vitals
- •Stage 2: 1000-1500 mL or vital sign changes (HR >110, SBP <90, SpO2 <95)
- •Stage 3: >1500 mL or 2+ units RBC needed or unstable vitals
- •Stage 4: cardiovascular collapse / massive transfusion
Steps
- 1Stage 1: bimanual uterine massage + IV access ×2 + oxytocin infusion
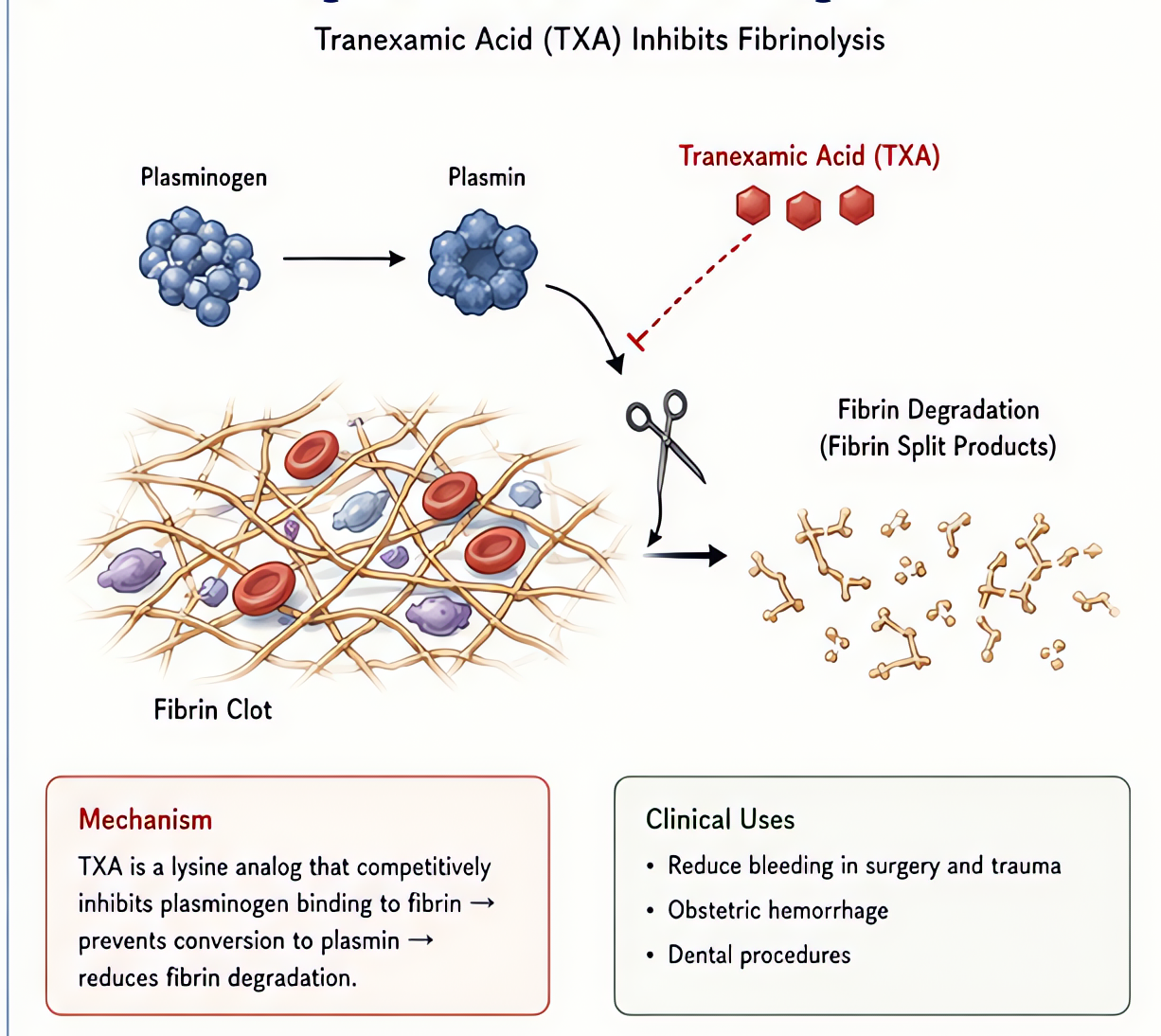
- 2Stage 2: activate OB hemorrhage team + escalate uterotonics + Foley + serial labsType/cross 4 units. Consider TXA 1g IV.
- 3Add carboprost (Hemabate) 250 mcg IMAVOID in asthma (bronchospasm). Repeat q15 min, max 2 mg.
- 4Add methylergonovine 0.2 mg IMAVOID in HTN, pre-eclampsia, coronary disease.
- 5Misoprostol 800-1000 mcg PR/SL/buccalSlower onset; useful alongside others.
- 6Bakri balloon or B-Lynch suture if atony refractory
- 7Stage 3: activate MTP, IR for embolization or surgical hysterectomy1:1:1 ratio + TXA + calcium repletion.
- 8Stage 4: massive transfusion + emergency hysterectomy + ICU
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Oxytocin | 10-40 U in 1L crystalloid IV (NEVER bolus — hypotension) | |
| Carboprost (Hemabate, PGF2α) | 250 mcg IM q15 min, max 2 mg — AVOID in asthma | |
| Methylergonovine (Methergine) | 0.2 mg IM q2-4h — AVOID in HTN/pre-eclampsia | |
| Misoprostol | 800-1000 mcg PR/SL/buccal | |
| TXA | 1g IV over 10 min within 3h, repeat 1g if continued bleeding | |
| Calcium chloride | 1g IV per 4 units PRBC (massive transfusion) |
Pitfalls
- !Carboprost in asthma → severe bronchospasm. Methergine in pre-eclampsia → hypertensive emergency. Choose by patient profile.
- !Oxytocin bolus → severe hypotension + tachycardia. Always run as infusion.
- !TXA window in OB is broader than trauma (WOMAN trial showed benefit up to 3h).
- !Don't underestimate concealed bleed — uterine atony with broad ligament hematoma may show stable BP until late.
Suggested reading
- ACOG SMI Hemorrhage Bundle 2022
- WOMAN Trial Lancet 2017
- Chestnut OB Anesthesia 6e
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.