Massive Transfusion / Hemorrhagic Shock
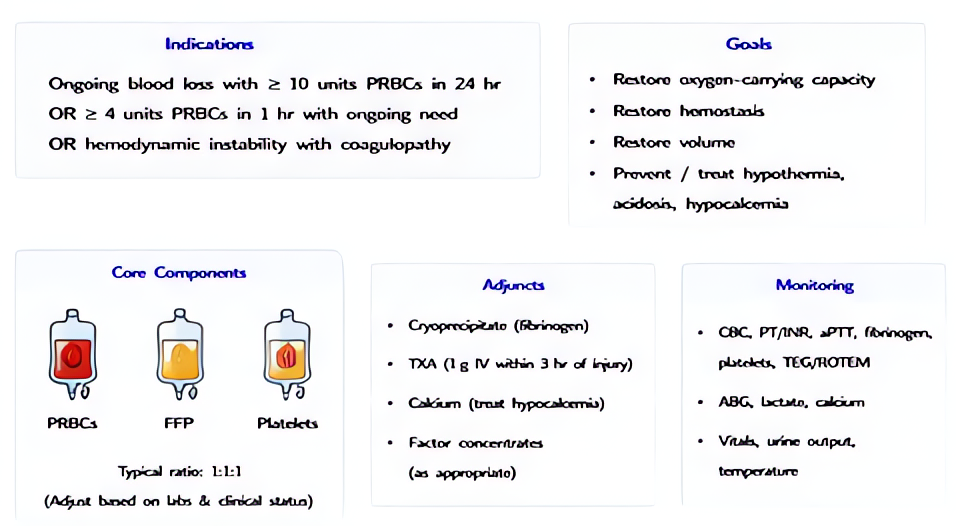
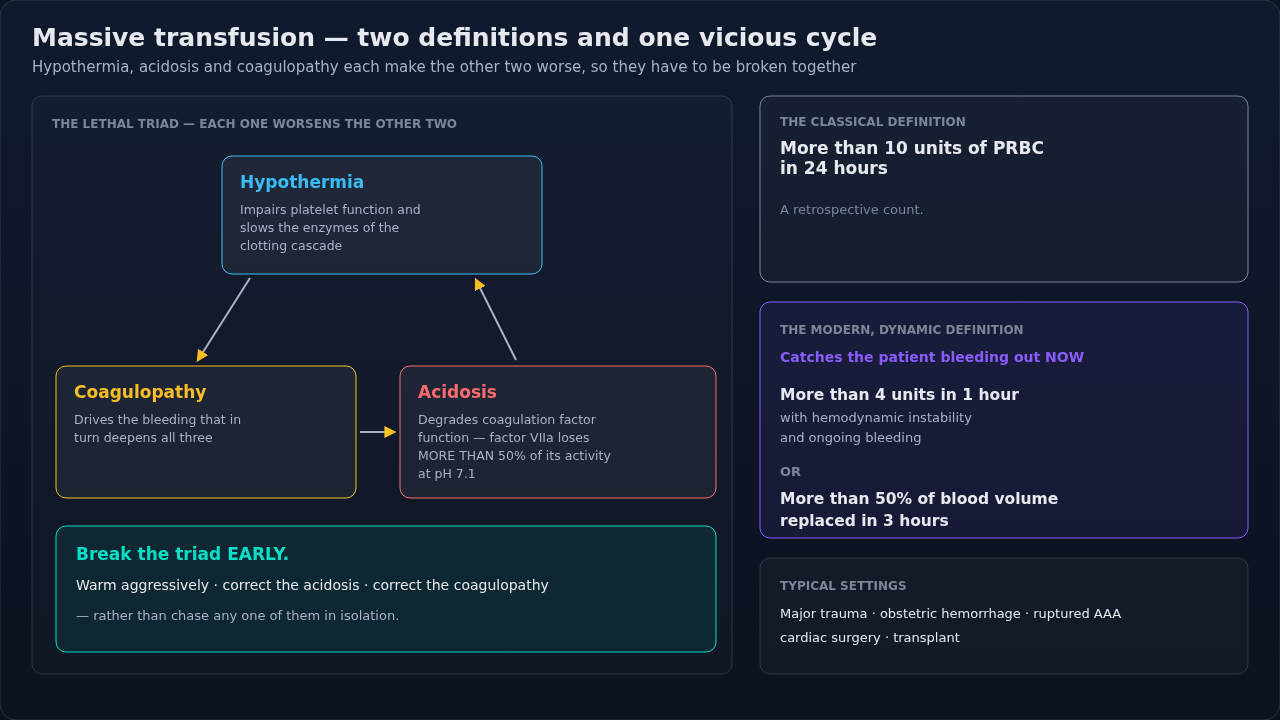
≥10 units PRBC in 24h or ≥4 units in 1h. Activate MTP early, give 1:1:1 ratio, treat lethal triad (hypothermia, acidosis, coagulopathy), use TXA within 3h, viscoelastic-guided component therapy.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •Hemorrhagic shock: SBP <90, HR >120, AMS, lactate >4
- •Anticipated >50% blood volume loss within 3h (ABC score, TASH score)
- •Trauma + class III/IV shock + ongoing bleeding
- •OB hemorrhage stage 2-3, ruptured AAA, GI bleed with instability
Steps
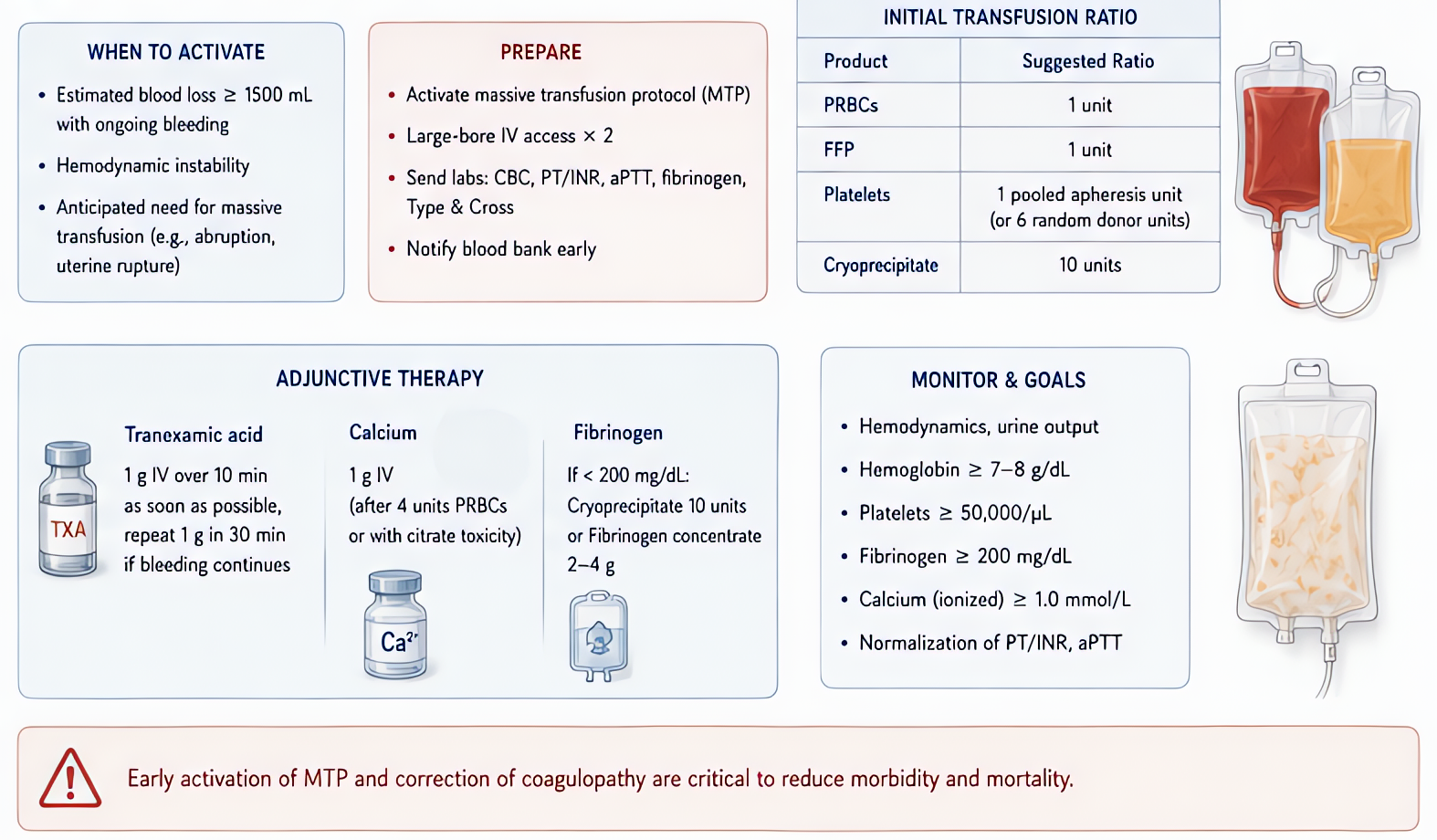
- 1Activate MTP — calls blood bank for pre-prepared 1:1:1 coolerMost institutional MTPs deliver 6 PRBC + 6 FFP + 1 platelet apheresis pack on first round.
- 2Two large-bore IVs (≥16g) or central access; warm fluids ≥38°C
- 3TXA 1g IV bolus (over 10 min) within 3h of injuryCRASH-2 mortality benefit if <3h; harm if >3h. Give second 1g infusion over 8h.
- 4Damage control resuscitation — permissive hypotension (SBP 80-90) until source controlled, EXCEPT in TBI (MAP ≥80)
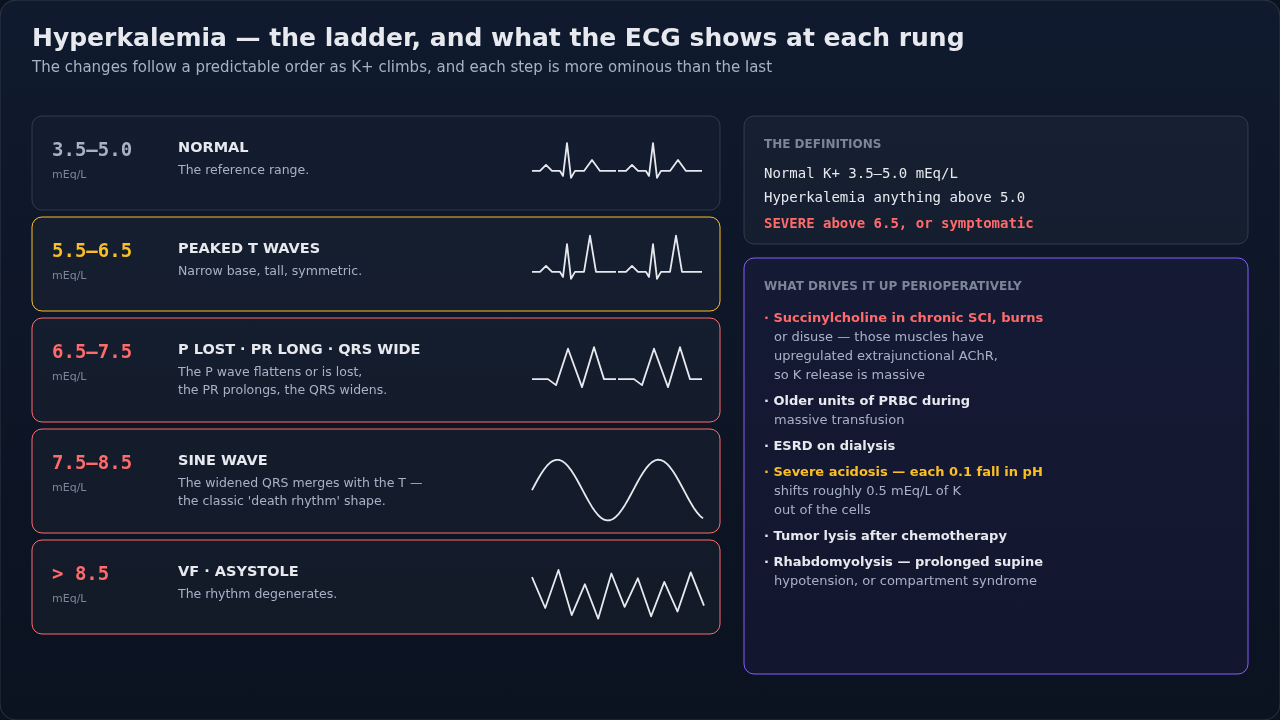
- 5Maintain calcium — 1g CaCl every 4 units PRBC (citrate chelation)
- 6Active warming — Bair Hugger, fluid warmer, raise OR temp
- 7Monitor: ABG q15 min, ionized Ca, fibrinogen (cryo if <150 trauma; OB threshold <200), TEG/ROTEM if availableCONTENT-AUDIT #1 (2026-06-10): OB-specific fibrinogen replacement threshold is <200 mg/dL during PPH per RCOG + Pacheco PPH algorithm + SMFM Consult 2015 -- fibrinogen falls earliest and predicts severity. Trauma threshold remains <150.
- 8Surgical/IR control of bleeding — definitive treatment
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Tranexamic acid (TXA) | 1g IV over 10 min, then 1g over 8h infusion | |
| Calcium chloride | 1g IV per 4 units PRBC | |
| Cryoprecipitate | 10 units if fibrinogen <150 mg/dL | |
| Prothrombin complex concentrate (PCC) | 25-50 units/kg for warfarin reversal or factor deficiency | |
| Recombinant factor VIIa | Last-resort (off-label); 90 mcg/kg |
Pitfalls
- !Don't wait for type-and-cross — use uncross-matched O-neg if female of childbearing age, O-pos otherwise.
- !TXA after 3h INCREASES mortality in trauma (CRASH-2). OB has wider window (WOMAN trial).
- !Permissive hypotension contraindicated in TBI — MAP ≥80 to maintain CPP.
- !Crystalloid >1L worsens coagulopathy — go straight to blood products.
- !Citrate intoxication = ionized Ca falls; check + replace empirically.
Suggested reading
- PROPPR Trial JAMA 2015
- CRASH-2 Lancet 2010
- WOMAN Trial Lancet 2017
- ASA Perioperative Hemorrhage Guidelines
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.