Intraoperative Myocardial Infarction / STEMI
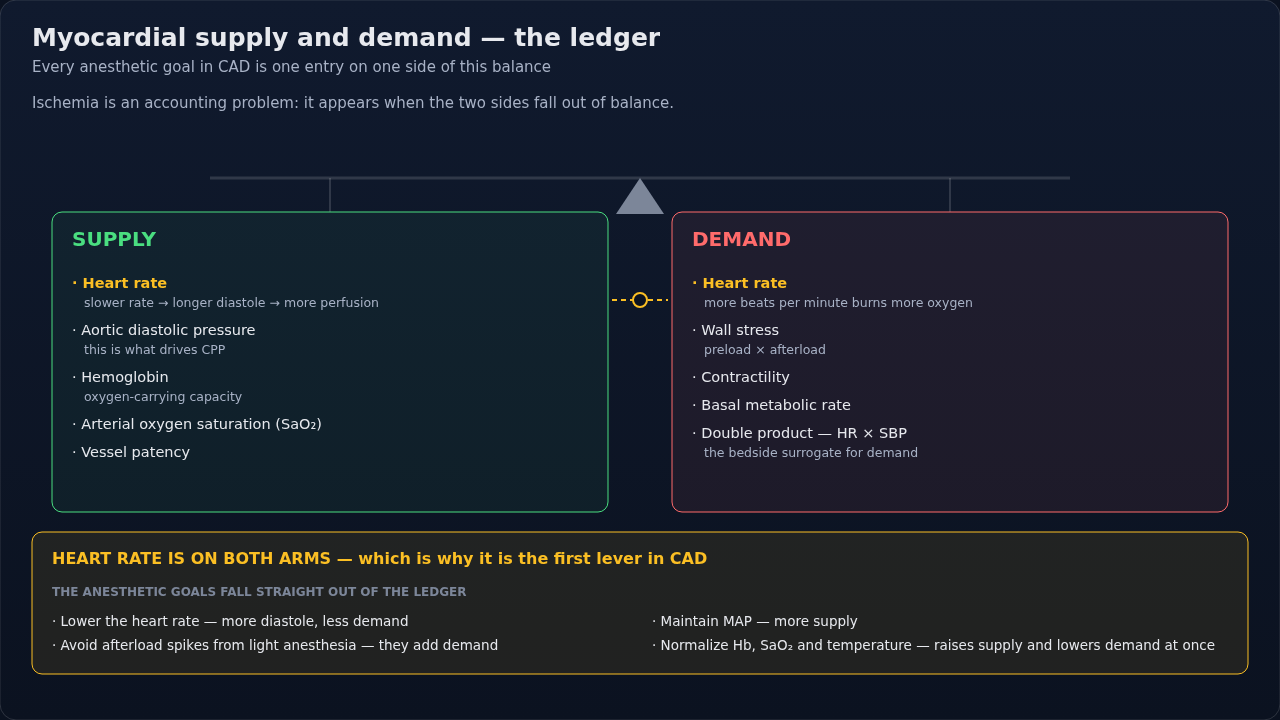
ST changes + hemodynamic instability + elevated troponin in OR. Optimize supply (O2, CPP) and demand (HR, contractility, afterload). Cardiology + cath lab consult; revascularization if STEMI.
⚡ Rehearsal mode
Walk the algorithm step by step
9 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •ST elevation ≥1 mm in 2 contiguous leads (II/III/aVF = inferior; V1-V4 = anterior; I/aVL/V5-V6 = lateral)
- •Sudden HD instability — hypotension, arrhythmia, new wall motion abnormality on TEE
- •Rising troponin + ST changes + clinical context
- •New LBBB + chest pain equivalent under anesthesia (Sgarbossa criteria)
Steps
- 1Increase FiO2 + optimize SpO2, ensure adequate Hgb (transfuse if <8)
- 2Treat hypotension — phenylephrine/NE to maintain coronary perfusionMAP ≥70 (or ≥80 if known CAD). Avoid tachycardia.
- 3Heart rate control — short-acting beta-blockerEsmolol bolus 10-20 mg → infusion 50-200 mcg/kg/min. Goal HR <70.
- 4Nitroglycerin if BP allows — 50-100 mcg IV bolus, infusion 0.25-1 mcg/kg/min
- 512-lead ECG + STAT troponin + cardiology consult
- 6Aspirin 325 mg PO/PR/NG if surgical site allowsRisk-benefit with surgical bleeding context.
- 7Heparin if STEMI confirmed + revascularization plannedSurgical bleeding context dictates timing.
- 8Cath lab activation for STEMI — primary PCI within 90 minContinue surgery vs abort depends on operative situation.
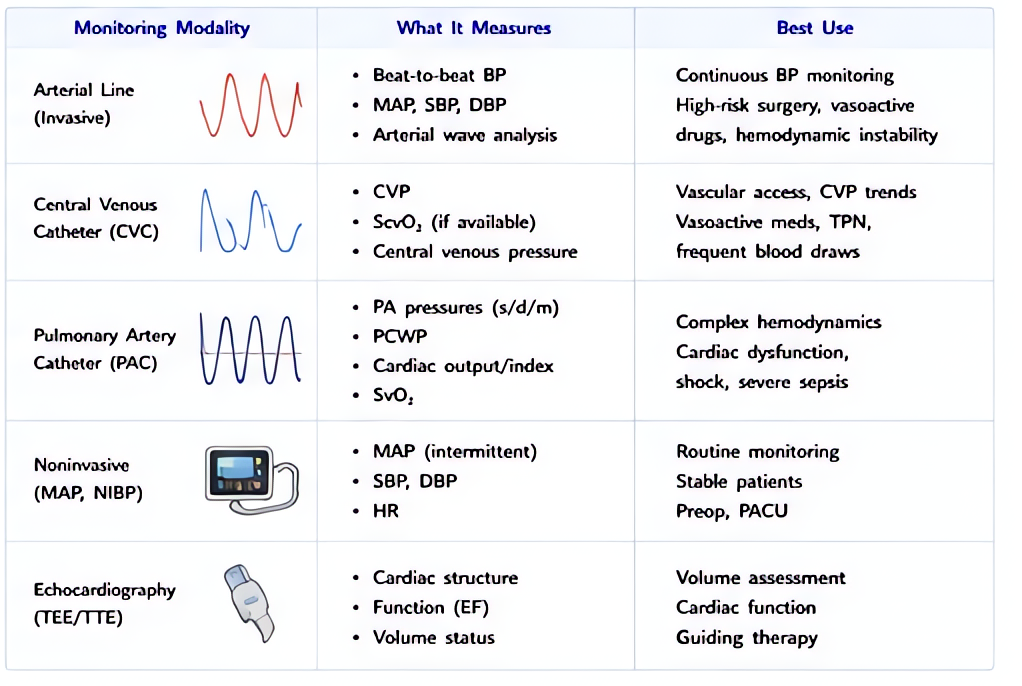
- 9TEE — wall motion abnormality, ejection fraction, complications (papillary muscle rupture, septal defect)
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Aspirin | 325 mg PO/PR (or 162 mg if recent dose) | |
| Nitroglycerin | 50-100 mcg IV bolus; infusion 0.25-1 mcg/kg/min (avoid if SBP <90) | |
| Esmolol | 10-20 mg IV bolus; infusion 50-200 mcg/kg/min | |
| Heparin | 60 U/kg bolus + 12 U/kg/hr (target aPTT 1.5-2.5×) — surgical context dependent | |
| Phenylephrine | 100 mcg IV bolus; infusion 0.5-2 mcg/kg/min | |
| Norepinephrine | 0.05-0.5 mcg/kg/min infusion if shock |
Pitfalls
- !Tachycardia + hypotension = double hit on coronary perfusion. Treat both.
- !Aspirin/heparin loading depends on surgical bleeding stage — discuss with surgeon.
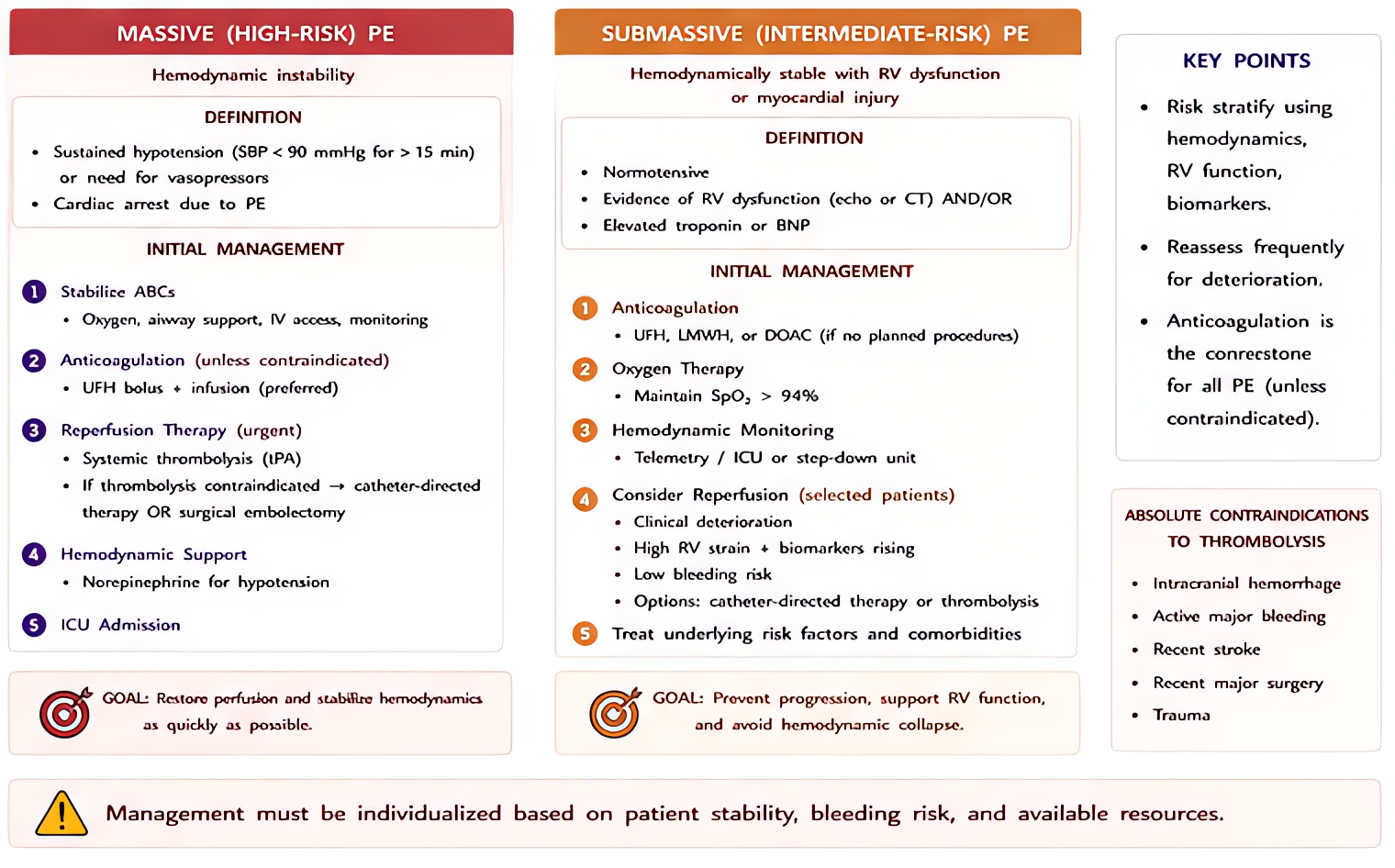
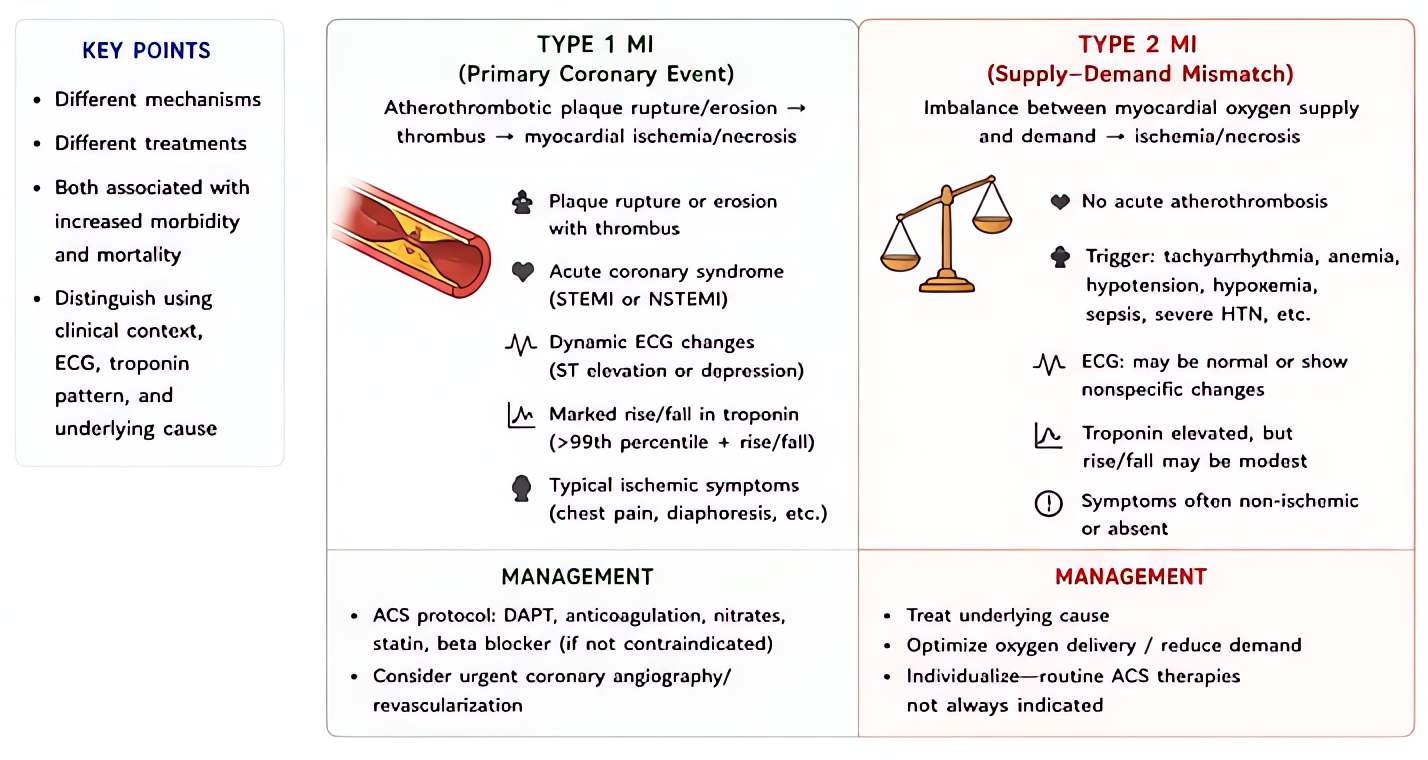
- !Type II MI (supply-demand mismatch) more common intraop than plaque rupture.
- !Don't extubate hypothermic, tachycardic, or hypertensive patient with active ischemia.
Suggested reading
- AHA STEMI Guidelines 2013
- ACC/AHA Periop Cardiac Eval 2014
- Miller's 9e Ch 54
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.