Hyperkalemic Cardiac Arrest
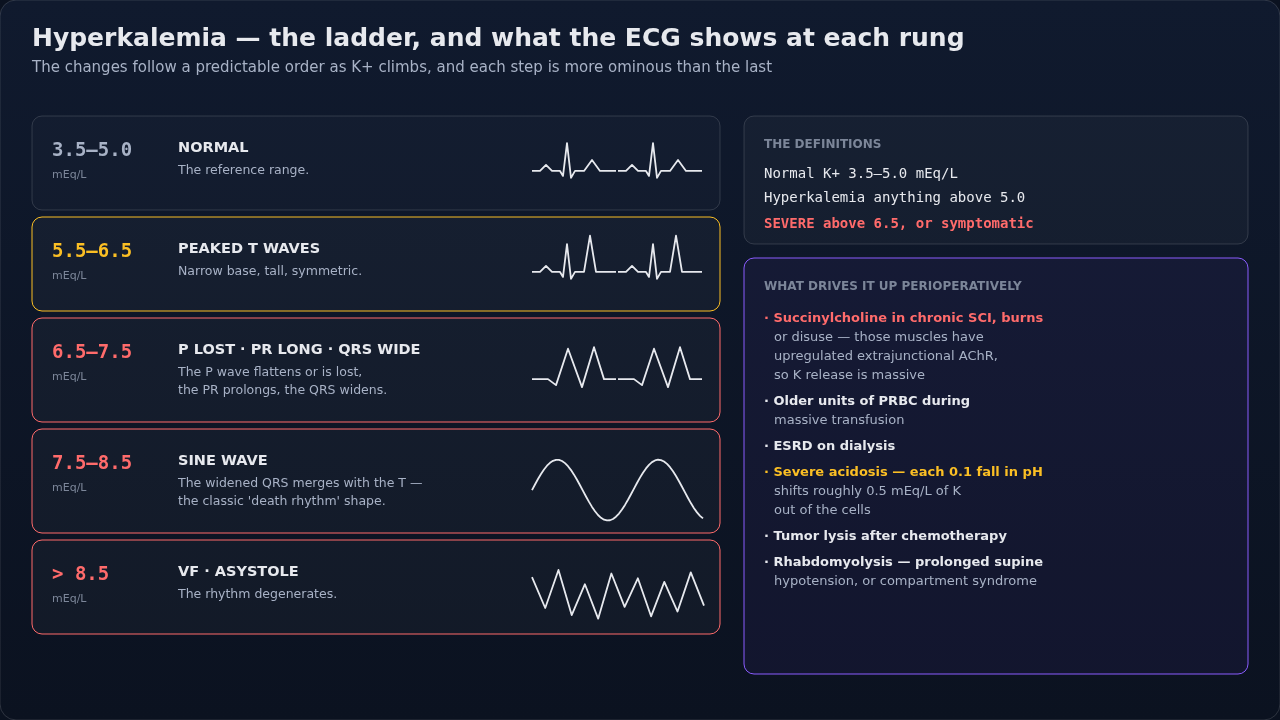
K+ >6.5 with ECG changes → CV collapse imminent. Calcium first (membrane stabilization), then drive K into cells, then remove from body. Common in ESRD, rhabdomyolysis, succinylcholine in burns/denervation, massive transfusion.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
- •ECG progression: peaked T waves → wide QRS → loss of P → sine wave → asystole/VF
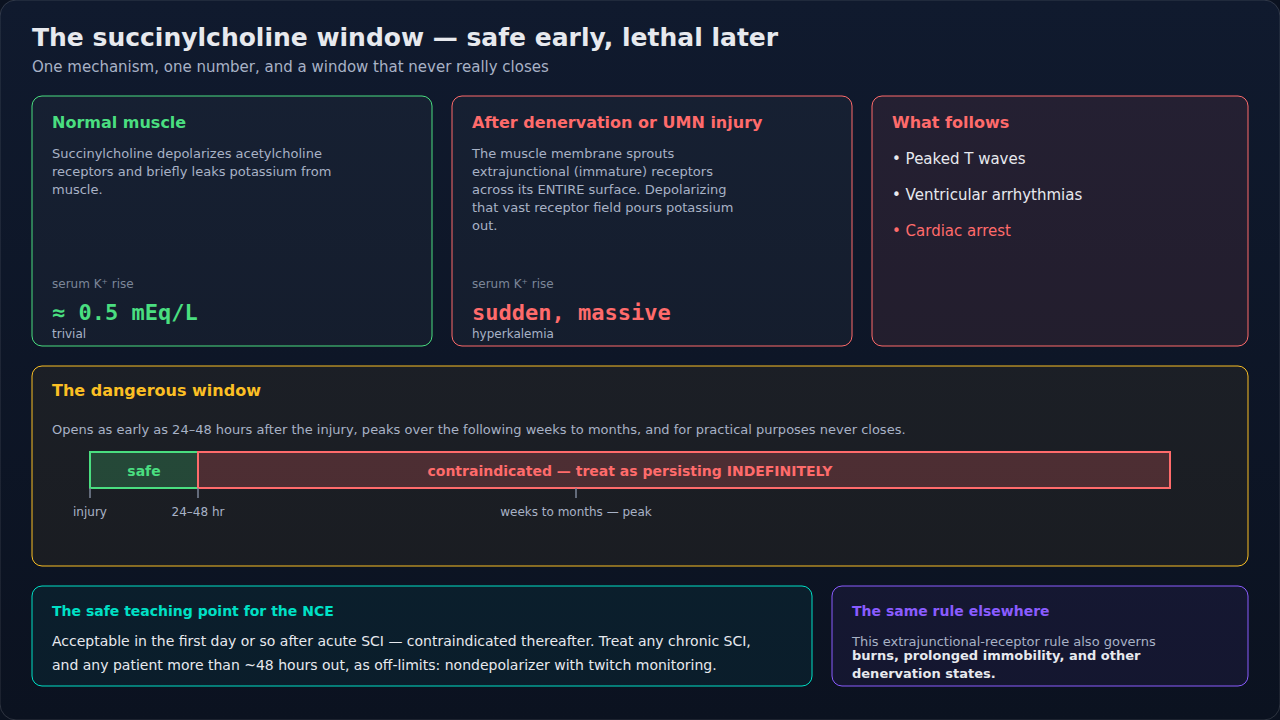
- •Setting: ESRD missing dialysis, rhabdomyolysis, crush injury, burns >24h, denervation, hemolysis, succinylcholine in susceptible patient
- •Massive transfusion (citrate + stored RBC K+) in cold, acidotic patient
Steps
- 1Calcium chloride 1g IV push (or 3g calcium gluconate)Stabilizes myocardial membrane in <3 min. Repeat q5 min if ECG persists.
- 2Insulin 10U regular IV + D50W 25g IVDrives K into cells; onset 15 min; check glucose hourly.
- 3Sodium bicarbonate 50 mEq IV (1 amp)Especially if acidotic. Slower than insulin.
- 4Albuterol 10-20 mg nebulizedAdjunct; peak effect 30-90 min. Beta-2 → K shift intracellularly.
- 5Hyperventilate to pH 7.5 (mechanical)Each 0.1 pH ↑ → K ↓ ~0.4 mEq/L. Temporizing only.
- 6Definitive removal — emergency hemodialysisMobilize nephrology + dialysis nurse simultaneously with above.
- 7Loop diuretic (furosemide 40-80 mg IV) if making urine
- 8Stop K+-elevating medications (succinylcholine, K-sparing diuretics, ACEi/ARB)
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Calcium chloride | 1g (10 mL of 10%) IV slow push via central line | |
| Calcium gluconate | 3g IV peripheral OK (less concentrated) | |
| Insulin (regular) | 10 units IV | |
| Dextrose 50% | 25-50g IV (1-2 amps) | |
| Sodium bicarbonate | 50-100 mEq IV bolus, then infusion | |
| Albuterol | 10-20 mg nebulized (4-5× standard asthma dose) | |
| Patiromer / SPS / Lokelma | After acute mgmt — for chronic K removal |
Pitfalls
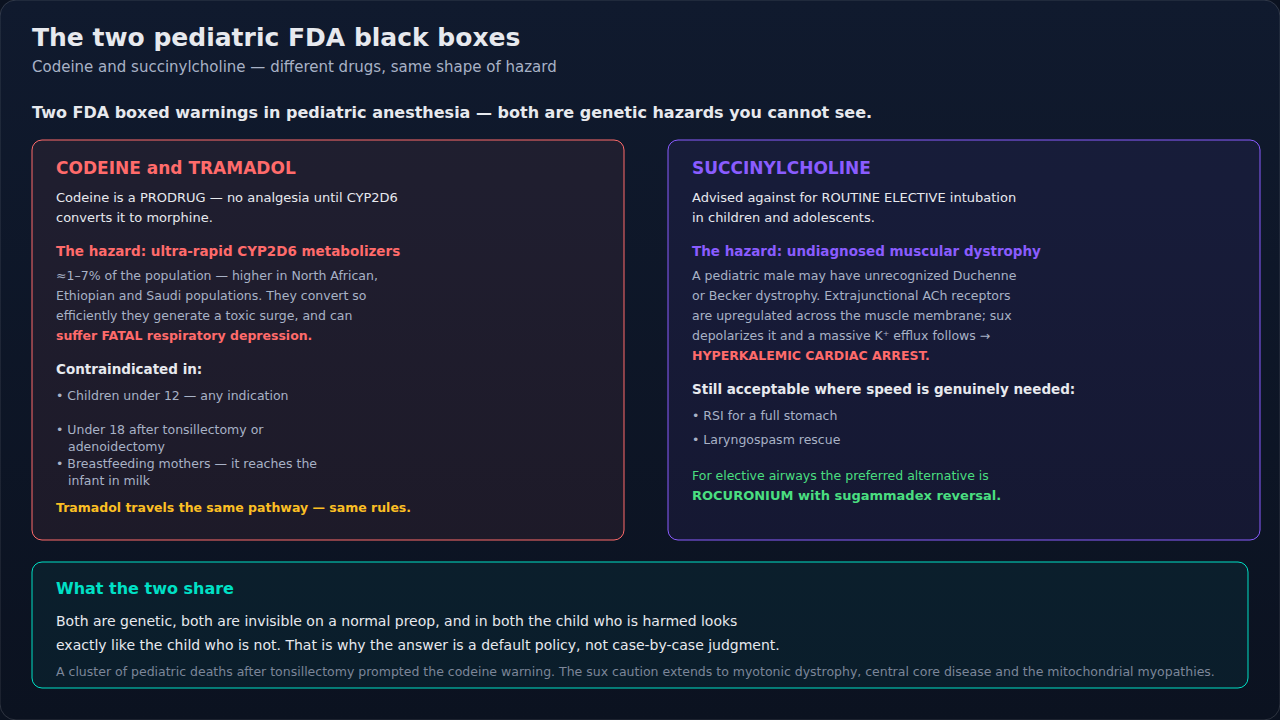
- !AVOID succinylcholine in known/suspected hyperK or risk groups (burns >24h, denervation, severe rhabdo).
- !Calcium does NOT lower K — it stabilizes the membrane. Still need K-lowering therapy.
- !Bicarbonate alone is unreliable; insulin/glucose more effective.
- !Dialysis is the only definitive treatment in ESRD.
Suggested reading
- KDIGO Acute Hyperkalemia 2024
- Marino ICU Book 5e
- Miller's 9e Ch 49
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.