Anticipated Difficult Airway — Pre-Induction Decision Tree
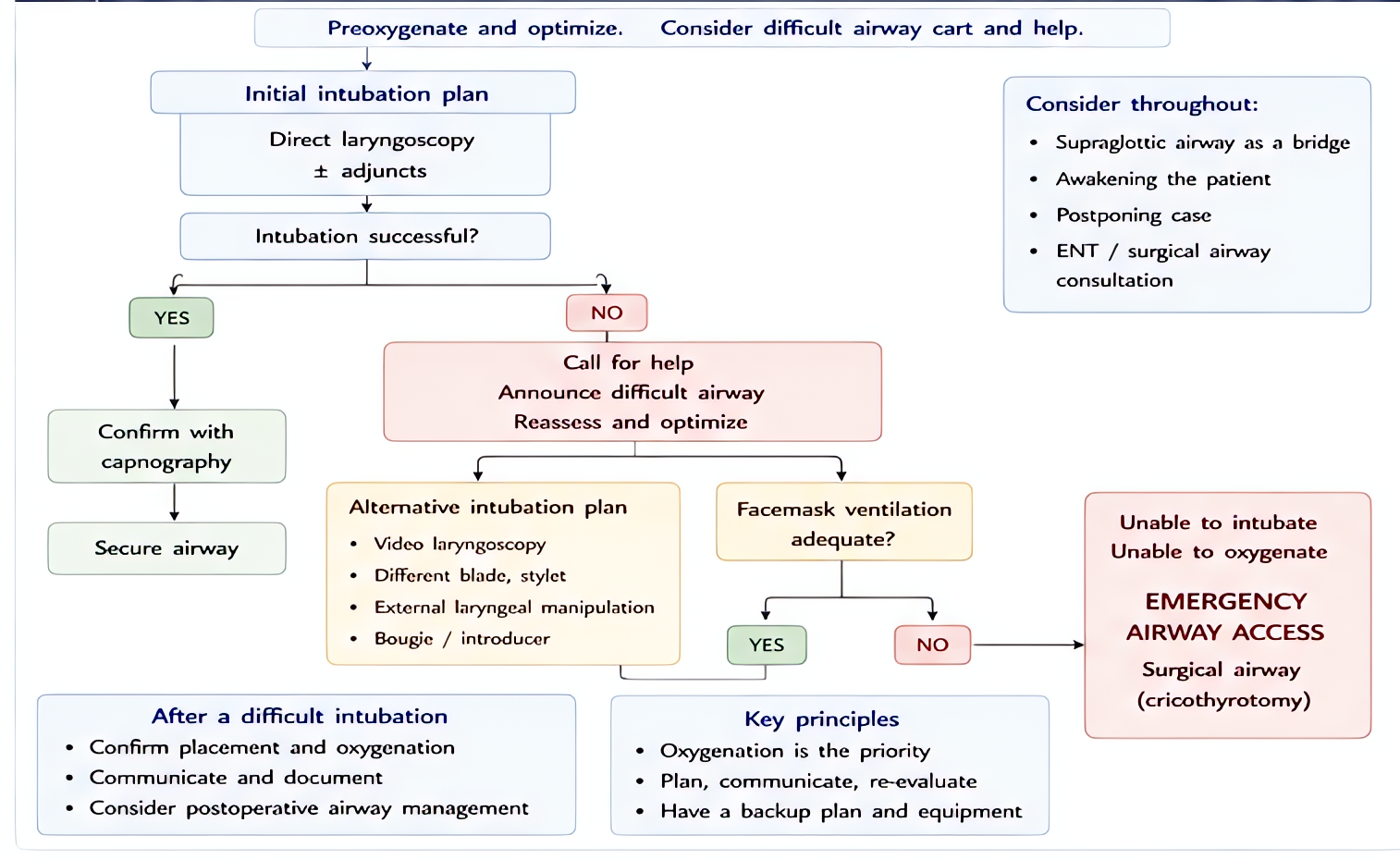
Pre-operative airway exam predicts difficulty. ASA Difficult Airway Algorithm 2022 emphasizes awake tracheal intubation when both ventilation and intubation are predicted difficult.
⚡ Rehearsal mode
Walk the algorithm step by step
8 steps · click-through one at a time. Forces you to pre-read each action before moving on — the way you should rehearse the real thing.
Recognition
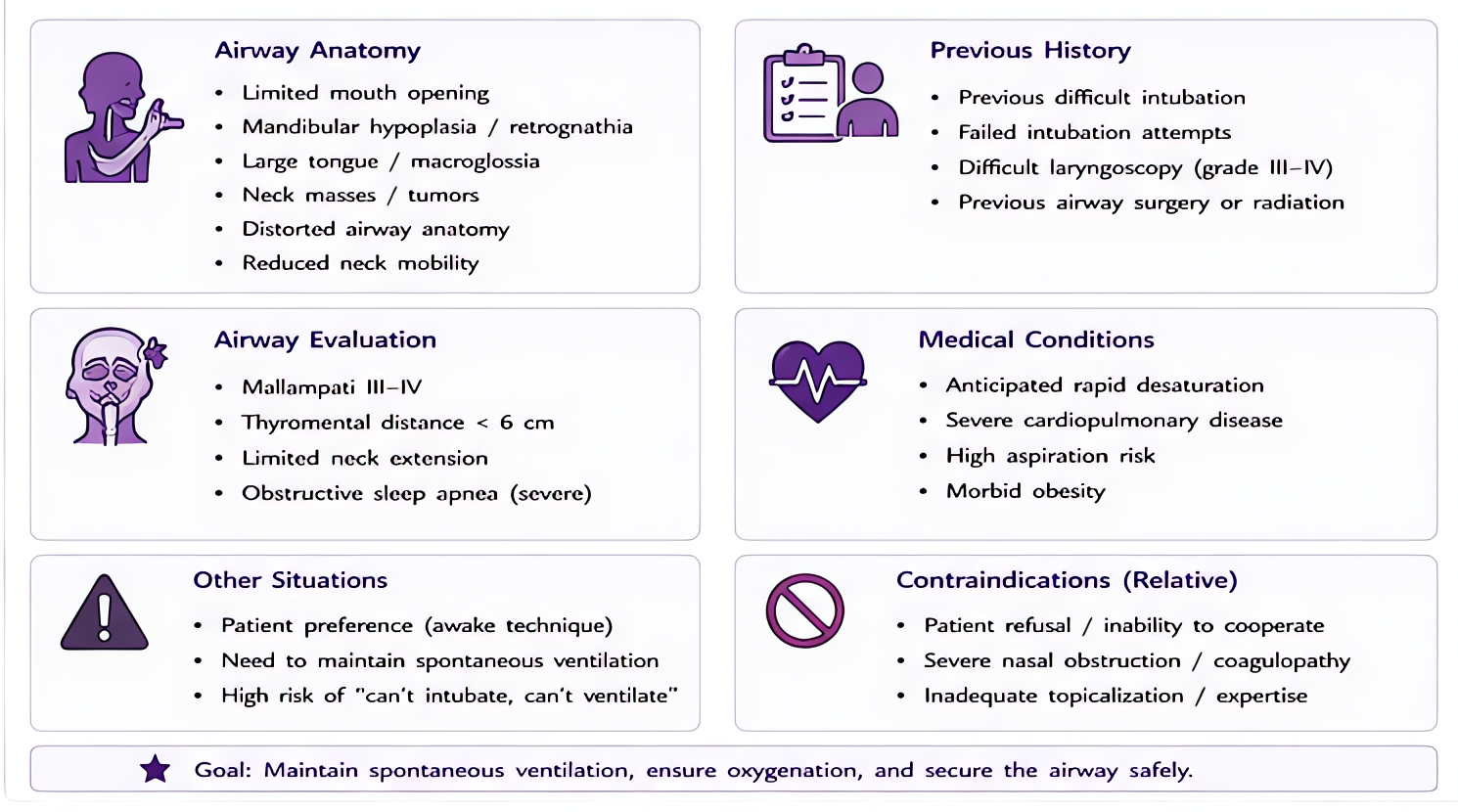
- •Mallampati III/IV + thyromental distance <6 cm + limited cervical extension
- •History of difficult airway or failed intubation
- •Syndromes (Pierre-Robin, Treacher-Collins, Down, MPS, achondroplasia)
- •Anatomic distortion — trauma, tumor, radiation, prior neck surgery
- •Restricted mouth opening <3 cm inter-incisor
Steps
- 1Pre-induction airway assessment + anesthesia + surgical plan + double-check rescue equipment
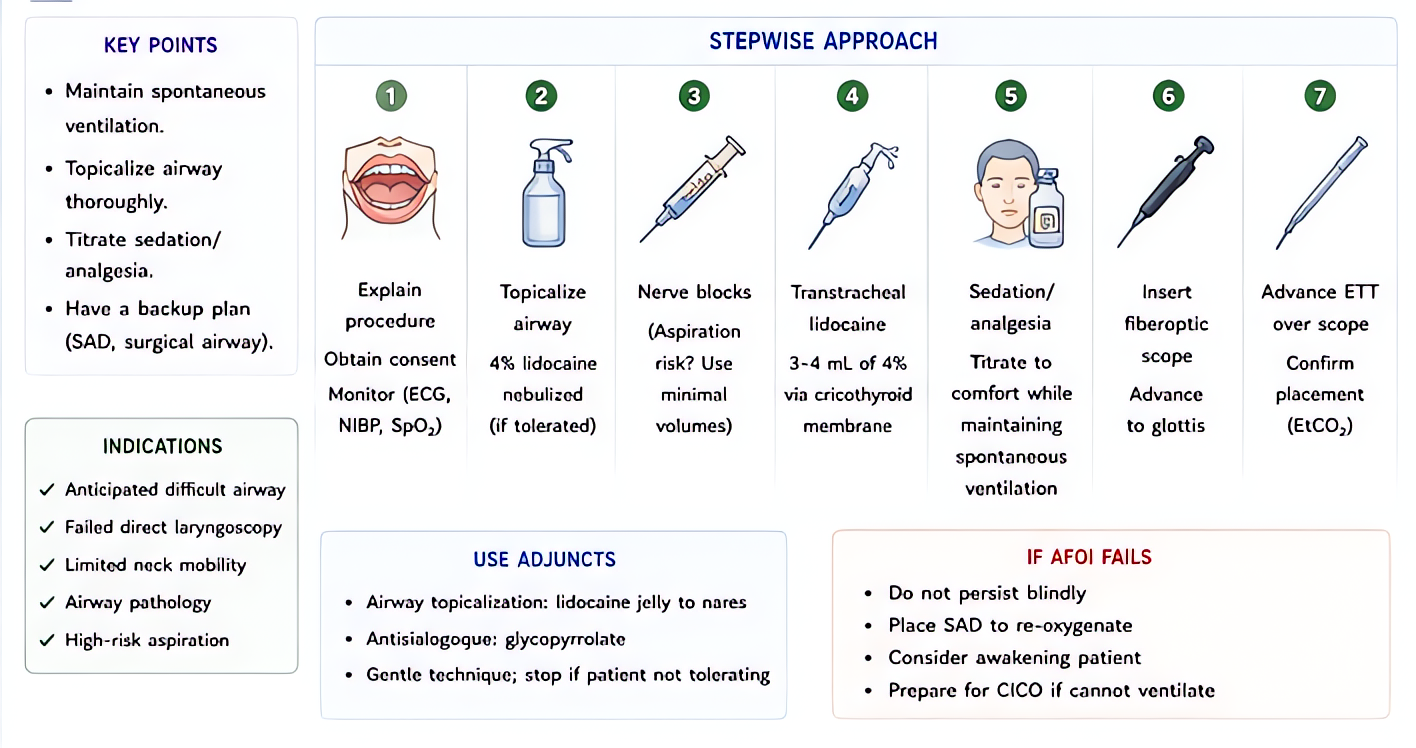
- 2Consider awake tracheal intubation if both DI and DV predictedTopicalize (lidocaine 4% nebulized + transtracheal + glossopharyngeal/superior laryngeal blocks); minimal sedation (dexmedetomidine, low-dose midaz/fent); fiberoptic or videolaryngoscope.
- 3If asleep: optimize position (ramped, ear-to-sternal-notch); pre-oxygenate to ETO2 ≥85%
- 4First attempt: video laryngoscopy preferred over direct in known difficult airway
- 5Limit attempts (max 3); each attempt risks bleeding + edema → CICO
- 6Always have rescue plan B ready — supraglottic device + bougie + cric kit visible/open
- 7Wake the patient up if unable + non-emergent (return to spontaneous ventilation)
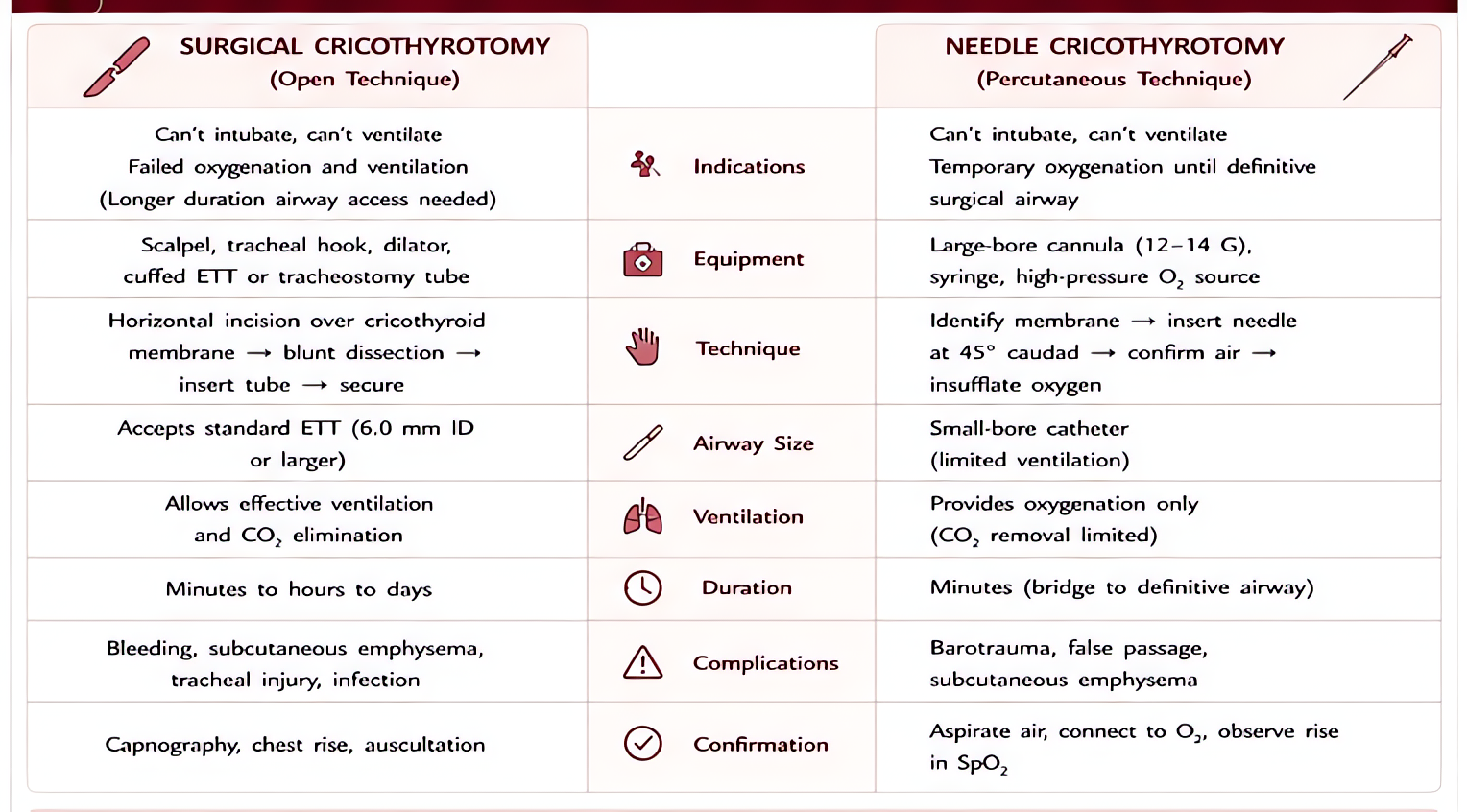
- 8If CICO — call for help, attempt SGA, then surgical/needle cric (see CVCI algorithm)
Drugs + doses
| Drug | Dose | Note |
|---|---|---|
| Lidocaine 4% nebulized | 4 mL nebulizer for awake topicalization | |
| Dexmedetomidine | 0.5-1 mcg/kg load over 10 min, 0.2-0.7 mcg/kg/hr maintenance | |
| Glycopyrrolate | 0.2 mg IV anti-sialogogue 15-30 min before awake intubation | |
| Sugammadex | 16 mg/kg IV for emergent rocuronium reversal if CICO |
Pitfalls
- !Don't paralyze before confirming you can ventilate (in unknown difficult airway).
- !Awake intubation requires patient cooperation — not for combative or hypoxic patients.
- !Repeated DL attempts cause hemorrhage + edema → can convert difficult to impossible.
- !Have a clear plan A/B/C and tell the team out loud.
Suggested reading
- ASA Difficult Airway Algorithm 2022
- DAS Guidelines 2015
- Miller's 9e Ch 44
Other crisis algorithms
- Malignant Hyperthermia (MH)
Hypermetabolic crisis triggered by volatile anesthetics or succinylcholine in genetically susceptible patients (RYR1, CACNA1S). Treat with dantrolene immediately.
- Perioperative Anaphylaxis
IgE-mediated (or pseudo-allergic) hemodynamic collapse from drug, latex, or transfusion exposure. Most common triggers in OR: NMBAs (rocuronium, succinylcholine), antibiotics, latex.
- Amniotic Fluid Embolism (AFE)
Rare, often fatal obstetric emergency — anaphylactoid syndrome of pregnancy. Sudden hemodynamic collapse, hypoxemia, and DIC during labor, delivery, or postpartum (within 30 min).
- LAST (Local Anesthetic Systemic Toxicity)
Cardiovascular and CNS toxicity from inadvertent IV injection or systemic absorption of local anesthetic. Bupivacaine highest cardiotoxicity. Ropivacaine + lidocaine slightly safer.
- Laryngospasm
Reflex closure of the vocal cords from light-anesthesia airway stimulation. Common in pediatrics, recent URI, and emergence. Untreated → hypoxia → bradycardia → arrest.
- High / Total Spinal
Cephalad spread of neuraxial local anesthetic causing apnea + cardiovascular collapse. Most common with epidural-to-subarachnoid migration in OB.