Phenytoin
Dilantin · Phenytek
Hydantoin sodium-channel-blocking antiepileptic
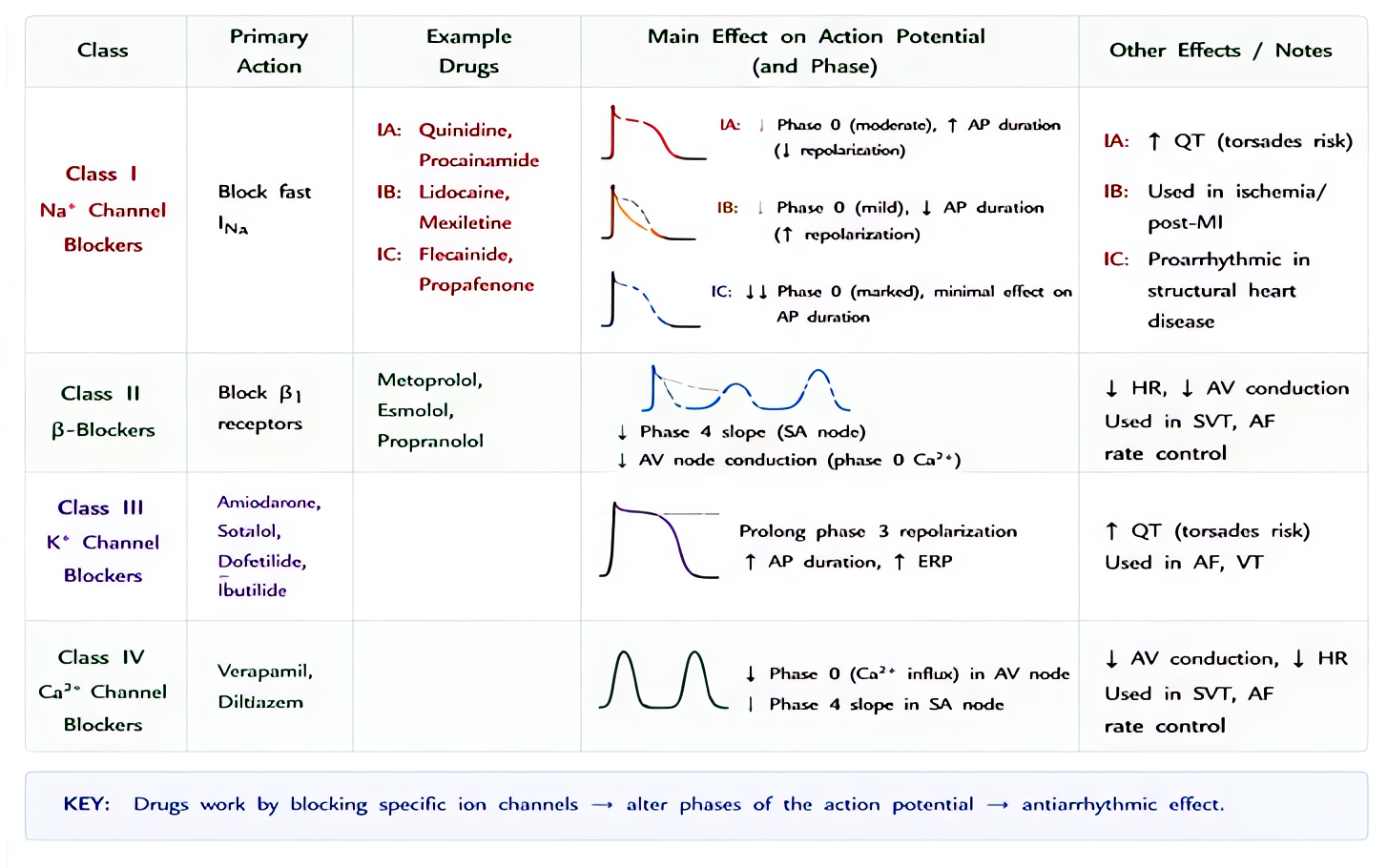
Use-dependent block of voltage-gated neuronal Na⁺ channels — stabilizes the inactivated state, raising the seizure threshold without affecting normal neuronal firing. Also blocks cardiac fast Na⁺ channels (class Ib antiarrhythmic activity).
Indications
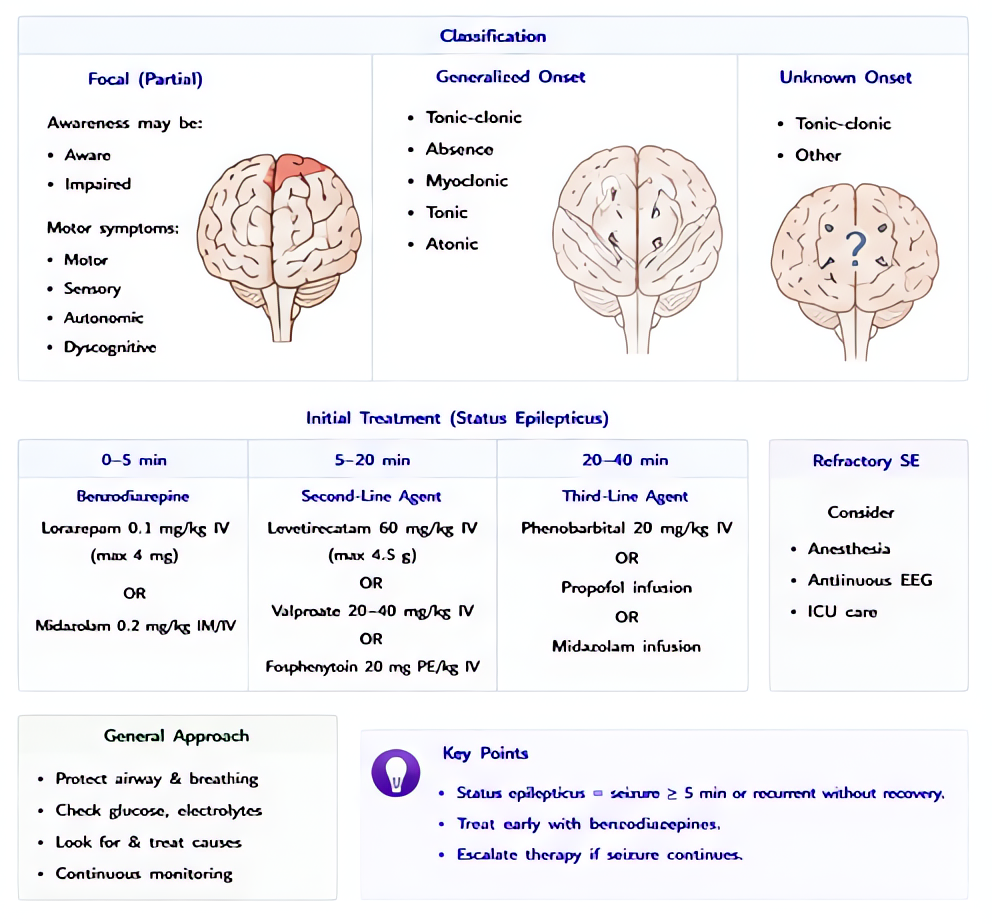
- •Status epilepticus (alternative second-line after benzo)
- •Generalized tonic-clonic + focal seizures (chronic)
- •Digoxin-induced ventricular arrhythmias (historical)
- •Trigeminal neuralgia (occasional second-line)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Status epilepticus loading | 20 mg/kg IV at ≤50 mg/min (≤25 mg/min in elderly/cardiac disease) | 20 mg/kg IV at ≤1 mg/kg/min |
| Maintenance | 100 mg IV/PO q8 h; titrate to level 10–20 mcg/mL (free 1–2 mcg/mL) | — |
| Fosphenytoin (preferred IV form) | 20 mg PE/kg IV at ≤150 mg PE/min — equivalent to 1.5× phenytoin dose in PE units; less infusion reaction | — |
Pharmacokinetics
Onset 0.5–1 h IV; peak 0.5–1 h. Half-life 7–42 h (zero-order kinetics — small dose change can produce large concentration change). 90% protein-bound (albumin); free fraction matters in hypoalbuminemia. Hepatic CYP2C9/CYP2C19 metabolism; potent CYP3A4 inducer.
Hemodynamic effects
Hypotension and bradycardia with rapid IV — limited by infusion rate and propylene-glycol vehicle (parenteral phenytoin only). Fosphenytoin lacks the propylene glycol and is hemodynamically safer.
Respiratory effects
Minimal direct effect; respiratory depression possible at toxic levels.
Side effects
- !Cardiovascular collapse with rapid IV (the propylene glycol vehicle, not the drug — fosphenytoin avoids this)
- !'Purple glove syndrome' — limb ischemia from extravasation; central line preferred
- !Nystagmus → ataxia → drowsiness → confusion as level rises (>20, >30, >40 mcg/mL respectively)
- !Gingival hyperplasia, hirsutism, coarsening of facies (chronic)
- !Stevens-Johnson syndrome / TEN — increased risk in HLA-B*1502 carriers (Asian ancestry — screen)
- !Hepatitis, lymphadenopathy (DRESS syndrome)
- !Megaloblastic anemia (folate deficiency), osteomalacia (vitamin D metabolism)
- !Fetal hydantoin syndrome (cleft palate, cardiac defects, microcephaly, hypoplastic nails)
Contraindications
- ×Sinus bradycardia, second/third-degree AV block, sinoatrial block
- ×Adams-Stokes syndrome
- ×Hypersensitivity to hydantoins
Clinical pearls
- ★FOSPHENYTOIN (Cerebyx) is the preferred parenteral form: water-soluble prodrug, faster infusion (150 mg PE/min vs 50), no propylene glycol → no cardiovascular collapse, can give IM, no purple-glove. Dose in 'phenytoin equivalents' (PE).
- ★FREE LEVEL IN LOW-ALBUMIN: corrected level = measured / (0.2 × albumin + 0.1) [Sheiner-Tozer]. In ICU patients with albumin 2.0, a measured 10 mcg/mL is actually a free fraction equivalent to 20 — at the toxic threshold.
- ★ENZYME INDUCTION: cuts warfarin, OCP, immunosuppressant (cyclosporine, tacrolimus), corticosteroid, NMB (rocuronium, vecuronium) levels. SRNAs see this clinically as paradoxically resistant non-depolarizing block in chronic phenytoin patients.
- ★ZERO-ORDER KINETICS: a 100 mg dose increase can move a level from 15 → 25 mcg/mL. Always recheck level 5–7 days after any change.
- ★ESETT (NEJM 2019): fosphenytoin equivalent to levetiracetam and valproate as benzo-refractory status second-line; choice driven by patient comorbidities.
Other drugs in Seizure Control
- Levetiracetam
Binds synaptic vesicle protein 2A (SV2A) and modulates neurotransmitter release; mechanism distinct from sodium-channel and GABA-receptor antiepileptics. Broad-spectrum efficacy against focal and generalized seizures.
- Valproate / Valproic Acid
Multimodal: enhances GABA synthesis (↑glutamic acid decarboxylase activity, ↓GABA-T degradation), blocks voltage-gated Na⁺ channels, and inhibits T-type Ca²⁺ channels in thalamic neurons. Broad-spectrum — covers focal, generalized, absence, and myoclonic seizures.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert