Levetiracetam
Keppra
SV2A vesicle-binding antiepileptic
Binds synaptic vesicle protein 2A (SV2A) and modulates neurotransmitter release; mechanism distinct from sodium-channel and GABA-receptor antiepileptics. Broad-spectrum efficacy against focal and generalized seizures.
Indications
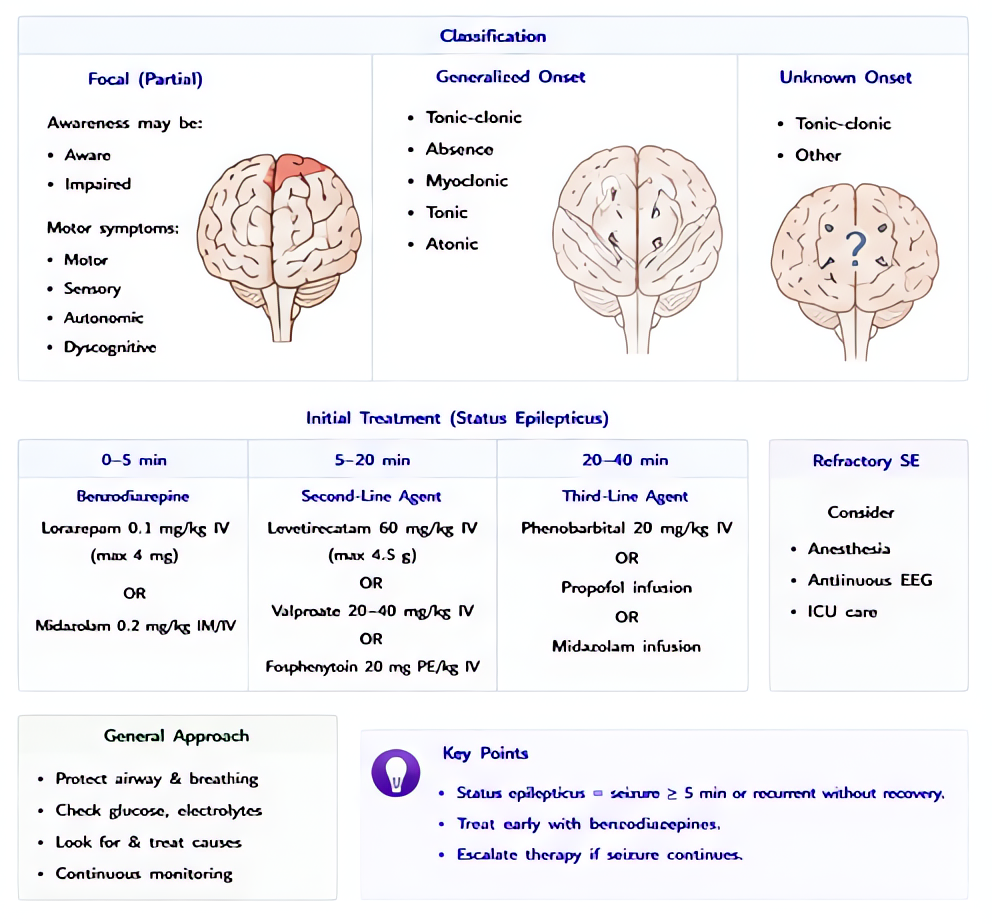
- •Status epilepticus (second-line per AAN/NCS guidelines after benzodiazepine)
- •Acute symptomatic seizure prophylaxis after TBI, intracranial surgery, SAH
- •Maintenance therapy for focal and generalized epilepsies
- •Postoperative seizure management when phenytoin contraindicated (cardiac, hepatic disease)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Status epilepticus IV load | 60 mg/kg (max 4.5 g) IV over 15 min — ESETT trial dose | 60 mg/kg (max 4.5 g) IV over 15 min |
| Postop seizure prophylaxis (TBI, craniotomy) | 500–1000 mg IV q12 h | — |
| Maintenance | 500–1500 mg PO/IV q12 h (max 3000 mg/day) | — |
Pharmacokinetics
IV onset minutes; oral bioavailability ~100%. Peak 1 h. Half-life 6–8 h (longer in renal impairment). 66% excreted unchanged in urine; minimal hepatic metabolism. No CYP induction or inhibition.
Hemodynamic effects
Minimal direct effect — preferred when hemodynamically labile.
Respiratory effects
Minimal effect.
Side effects
- !Somnolence, asthenia, dizziness (most common)
- !Behavioral effects: irritability, depression, suicidal ideation (boxed warning) — especially in patients with mood disorder history
- !Headache
- !Thrombocytopenia (rare)
- !Anaphylaxis / angioedema (very rare)
Contraindications
- ×Hypersensitivity to levetiracetam
Reversal / antidote
None — supportive; hemodialysis effective for overdose given high renal clearance and low protein binding.
Clinical pearls
- ★ESETT TRIAL (NEJM 2019): levetiracetam, fosphenytoin, and valproate showed equivalent efficacy as second-line agents in benzo-refractory status epilepticus. Levetiracetam is favored when cardiac or hepatic disease makes phenytoin or valproate risky.
- ★RENAL DOSING: CrCl 50–80 → 500–1000 mg q12 h; 30–50 → 250–750 mg q12 h; <30 → 250–500 mg q12 h; HD → 500–1000 mg q24 h with 250–500 mg supplement post-dialysis.
- ★NO ENZYME INDUCTION: doesn't accelerate metabolism of warfarin, OCPs, immunosuppressants — major advantage over phenytoin and carbamazepine in transplant and oncology patients.
- ★NEUROPSYCHIATRIC SCREEN: ask about depression, suicidal ideation, irritability before starting; counsel patient and family.
Other drugs in Seizure Control
- Phenytoin
Use-dependent block of voltage-gated neuronal Na⁺ channels — stabilizes the inactivated state, raising the seizure threshold without affecting normal neuronal firing. Also blocks cardiac fast Na⁺ channels (class Ib antiarrhythmic activity).
- Valproate / Valproic Acid
Multimodal: enhances GABA synthesis (↑glutamic acid decarboxylase activity, ↓GABA-T degradation), blocks voltage-gated Na⁺ channels, and inhibits T-type Ca²⁺ channels in thalamic neurons. Broad-spectrum — covers focal, generalized, absence, and myoclonic seizures.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert