Cisatracurium
Nimbex
Benzylisoquinolinium non-depolarizing neuromuscular blocker (intermediate duration)
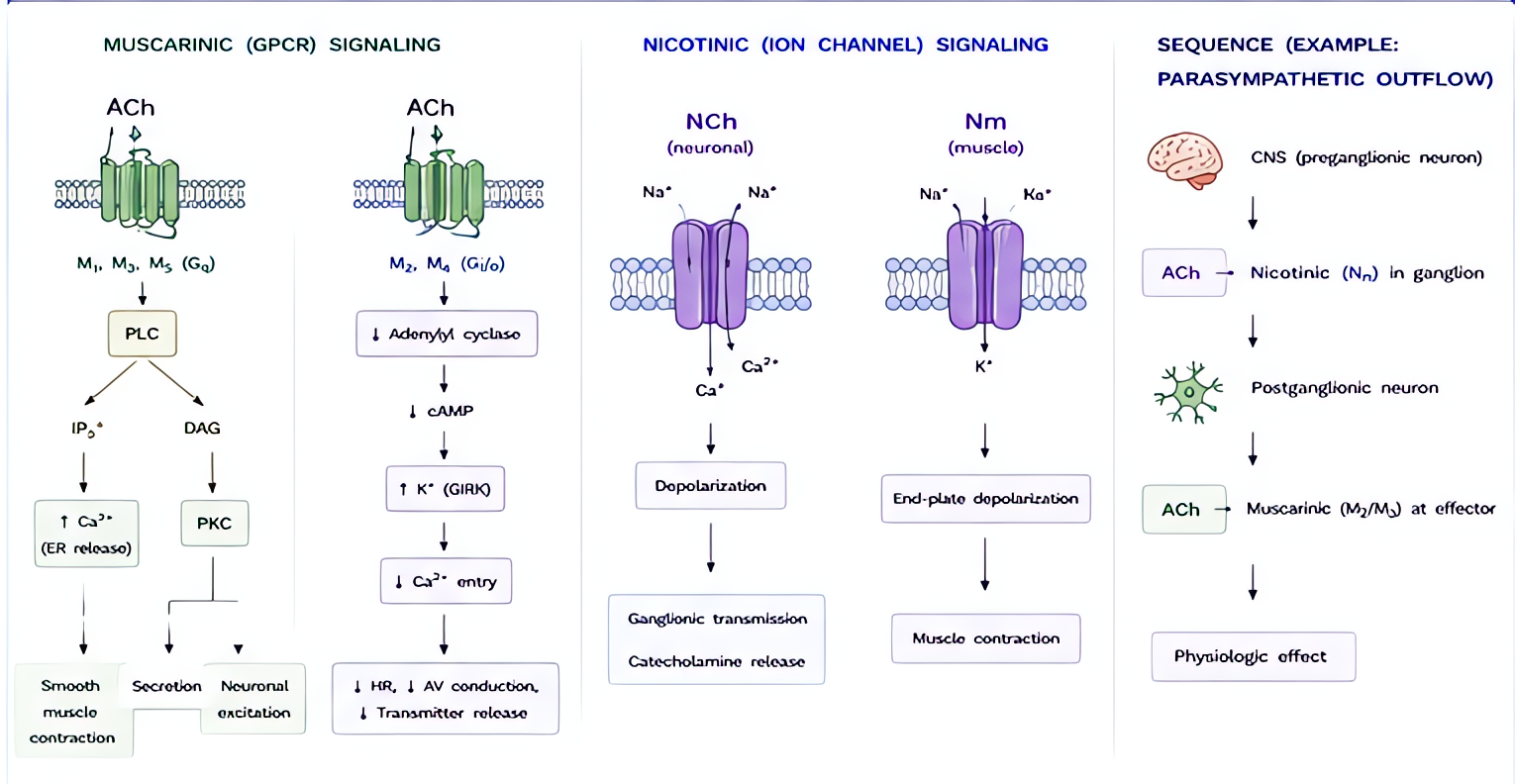
Competitive antagonist at the post-synaptic nicotinic ACh receptor at the neuromuscular junction. Single cis-cis isomer of atracurium (4× more potent, lower laudanosine production).
Indications
- •Neuromuscular blockade for intubation + maintenance
- •Preferred when renal/hepatic dysfunction, patients without IV access for sugammadex, organ donor procurement
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Intubation (3–4× ED95) | 0.15–0.20 mg/kg IV | 0.10–0.15 mg/kg IV (age 2–12) |
| Maintenance bolus | 0.03 mg/kg IV q20–30 min | — |
| Continuous infusion | 1–3 mcg/kg/min after recovery to T1 | 1.0–2.0 mcg/kg/min |
Pharmacokinetics
Onset 2–3 min (slower than rocuronium 1–2 min). Duration of intubating dose ~45–60 min. Eliminated by HOFMANN ELIMINATION (spontaneous, pH+temperature-dependent breakdown in plasma at body pH/37°C). Independent of hepatic + renal clearance — the unique property that drives ICU + organ-failure use. Hofmann produces laudanosine (CNS stimulant at very high cumulative doses; clinically irrelevant with cis vs older atracurium).
Hemodynamic effects
Hemodynamically inert at clinical doses — no significant histamine release (unlike older atracurium), no autonomic effects, no HR/BP changes. The cleanest cardiovascular profile of any NMB.
Side effects
- !Slower onset than rocuronium (not preferred for true RSI)
- !No sugammadex reversal — must wait for spontaneous recovery or use neostigmine
- !Laudanosine accumulation with very prolonged infusions (days) — theoretical seizure risk, not seen clinically with cis
- !Slight precipitation with alkaline drugs (propofol) — flush line between
Contraindications
- ×Known hypersensitivity (rare)
Reversal / antidote
Neostigmine 0.04–0.07 mg/kg IV + glycopyrrolate 0.01 mg/kg (or atropine) once TOF count ≥ 2/4. Sugammadex DOES NOT reverse cisatracurium (only aminosteroids: roc, vec, panc).
Clinical pearls
- ★Drug of choice when both renal AND hepatic function are impaired or unknown (organ failure ICU patient, transplant recipient, sepsis with multi-organ dysfunction).
- ★Hofmann elimination: NMB clearance unaffected by perfusion, hepatic blood flow, dialysis status — predictable offset.
- ★ED95 ~0.05 mg/kg; intubating dose is 2–4× ED95; bolus + infusion strategy avoids histamine that older atracurium produced.
- ★Stored refrigerated (4°C); discard if shaken vigorously or warmed > 25°C × prolonged period (Hofmann begins in the syringe).
- ★If you need RSI (60-sec onset) AND sugammadex reversibility: use rocuronium, not cisatracurium.
Other drugs in Muscle Relaxants & Reversals
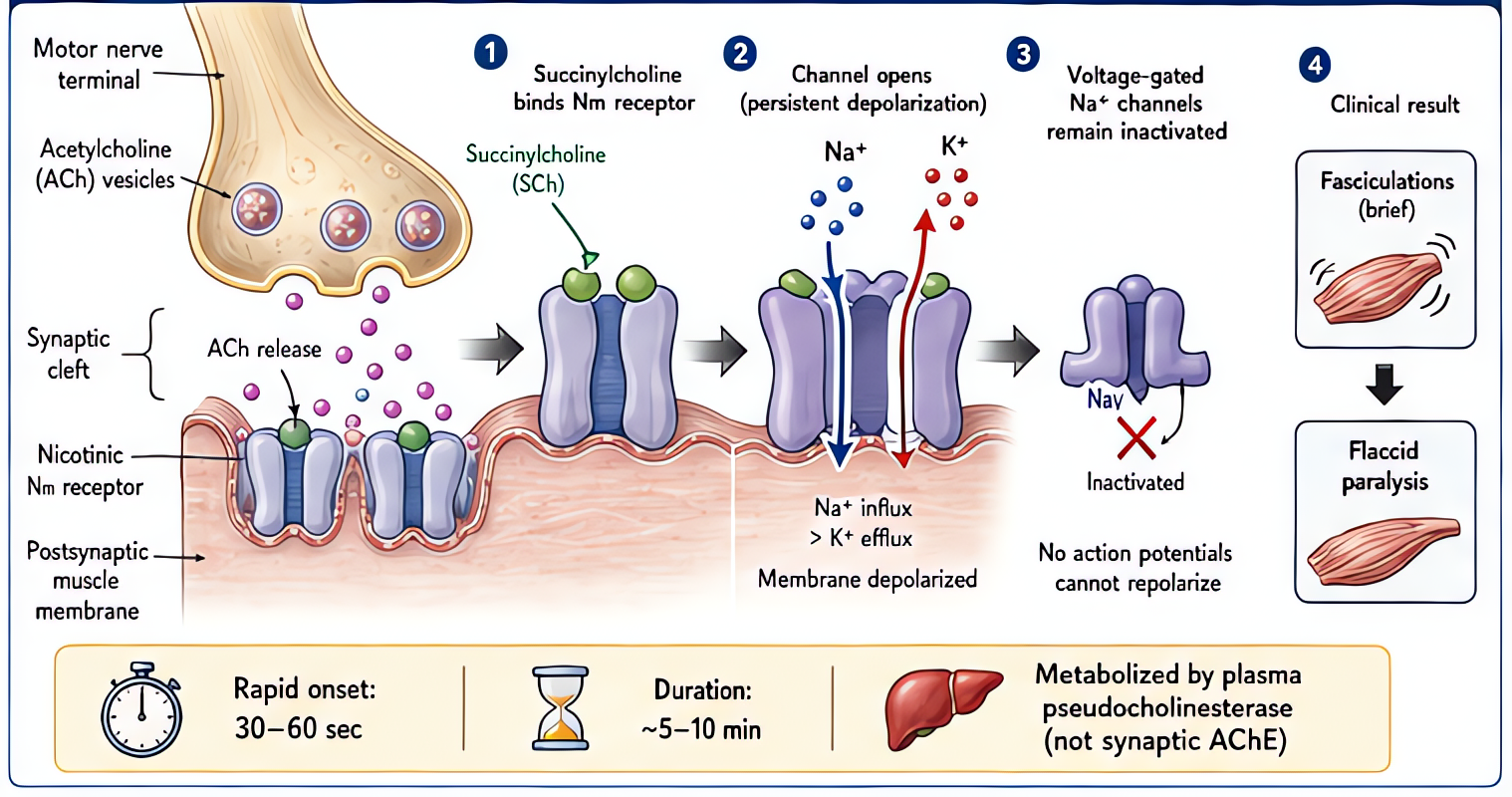
- Succinylcholine
Acetylcholine receptor agonist at the NMJ; sustained depolarization → fasciculations → flaccid paralysis. Hydrolyzed by plasma cholinesterase.
- Rocuronium
Competitive antagonist at the NMJ nicotinic receptor.
- Sugammadex
Encapsulates rocuronium > vecuronium > pancuronium in 1:1 complex. No effect on cisatracurium, atracurium, sux.
- Vecuronium
Competitive nicotinic ACh-receptor antagonist at the NMJ. Aminosteroid → reversible by sugammadex.
- Atracurium
Competitive nicotinic antagonist. Eliminated by HOFMANN elimination (spontaneous, temp/pH-dependent) + ester hydrolysis → organ-independent clearance.
- Pancuronium
Competitive nicotinic antagonist. Also blocks cardiac muscarinic receptors (vagolytic) → tachycardia.
- Mivacurium
Competitive nicotinic antagonist. UNIQUE among non-depolarizers: metabolized by PLASMA CHOLINESTERASE (like succinylcholine) → shortest-acting NDMR.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert