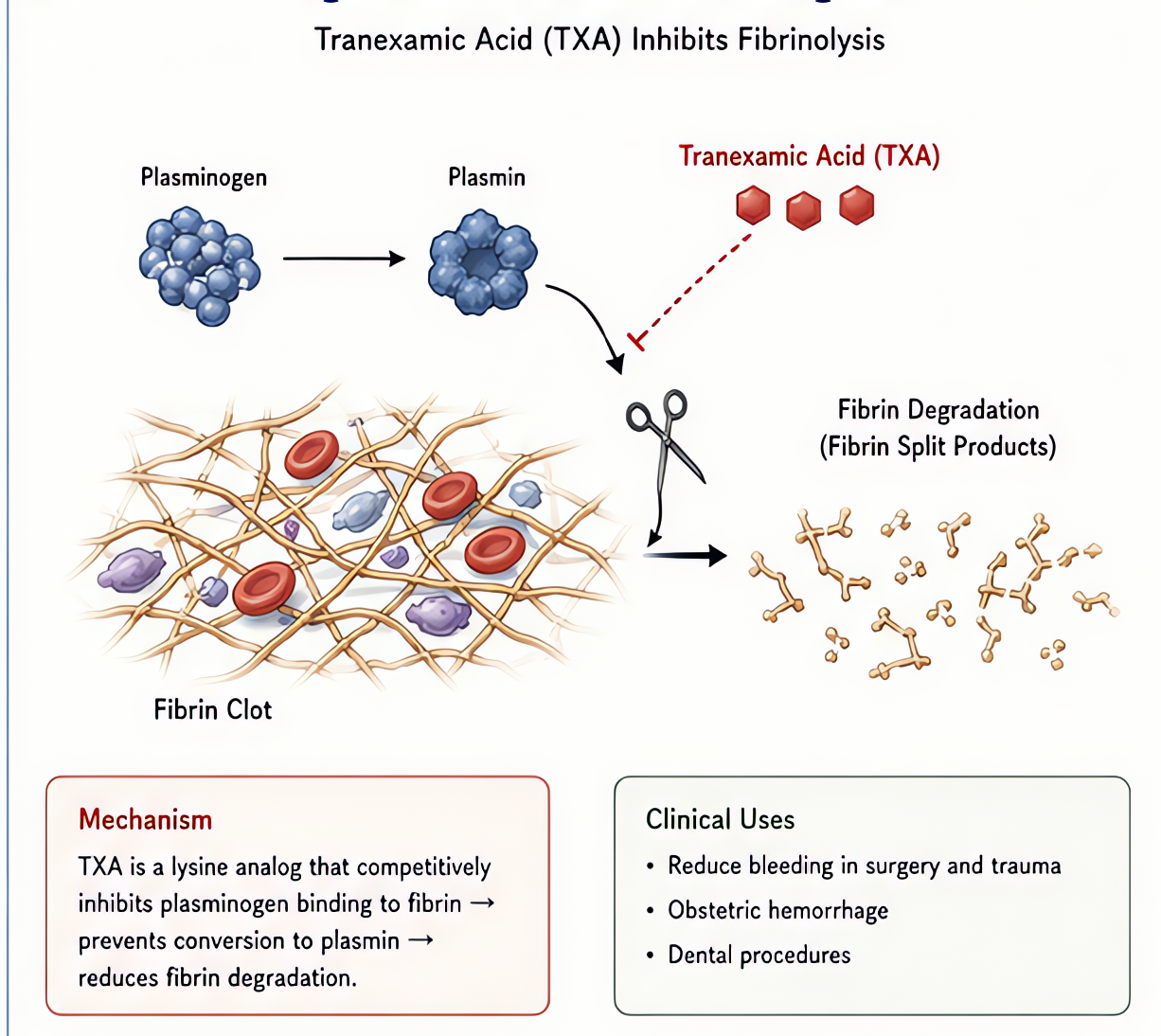
Tranexamic Acid (TXA)
Cyklokapron · Lysteda
Antifibrinolytic (lysine analog)
Reversibly binds plasminogen, blocking conversion to plasmin → preserves fibrin clot.
Indications
- •Trauma (CRASH-2: ↓mortality if given < 3 h post-injury)
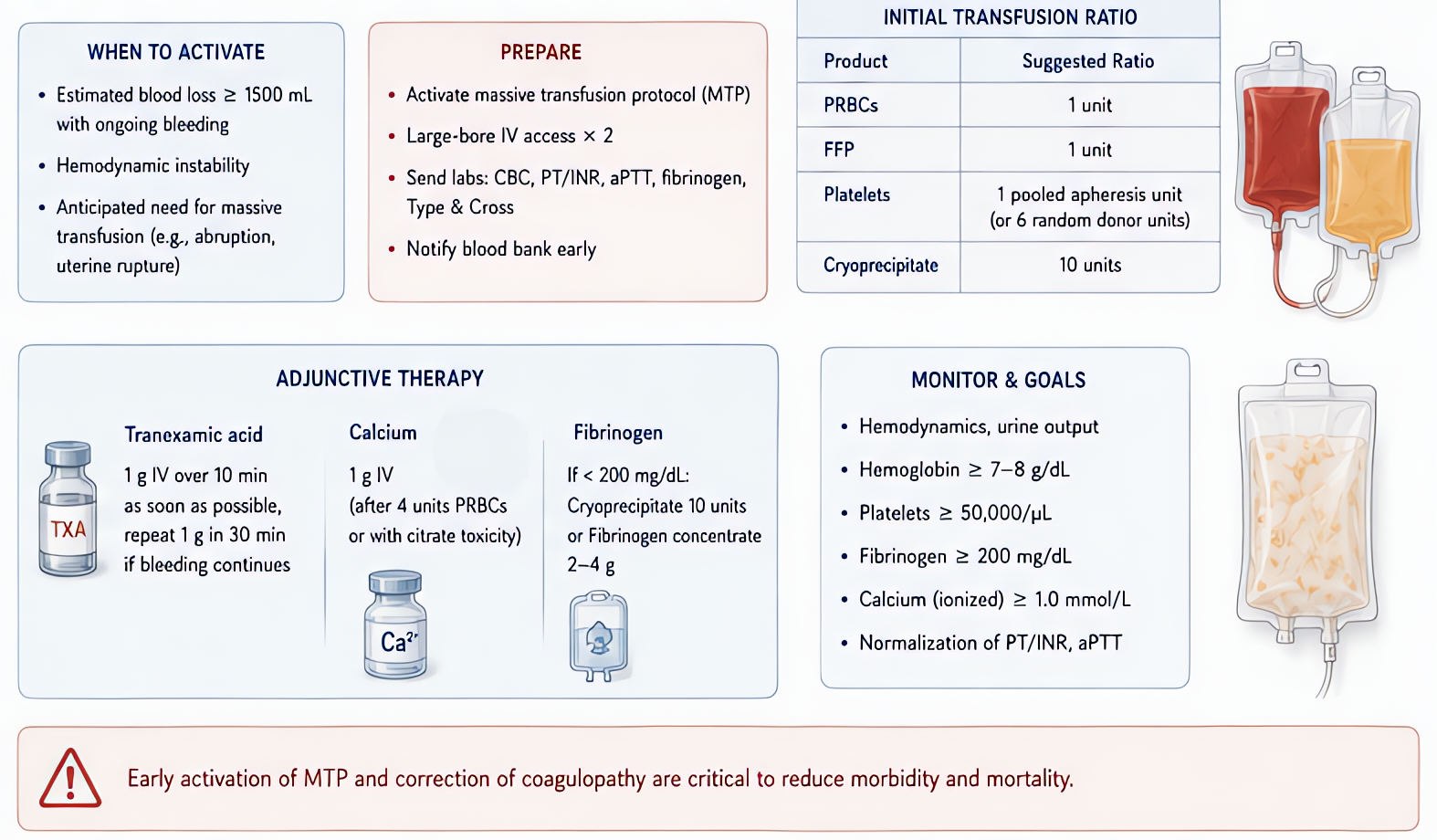
- •Postpartum hemorrhage (WOMAN trial)
- •Cardiac surgery + bypass
- •Orthopedic (joint replacement)
- •Heavy menstrual bleeding
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Trauma | 1 g IV over 10 min, then 1 g over 8 h | — |
| PPH | 1 g IV over 10 min; repeat at 30 min if continued bleeding | — |
| Cardiac surgery | 10–30 mg/kg load + 1–16 mg/kg/hr infusion (varies) | — |
| Joint replacement | 10–20 mg/kg IV at incision + closure | — |
Pharmacokinetics
Onset 5–15 min. Renal excretion.
Side effects
- !Seizures (high-dose, especially in cardiac surgery — GABA-A inhibition)
- !Visual disturbance
- !Thromboembolism (theoretical risk; not seen consistently in trials)
Contraindications
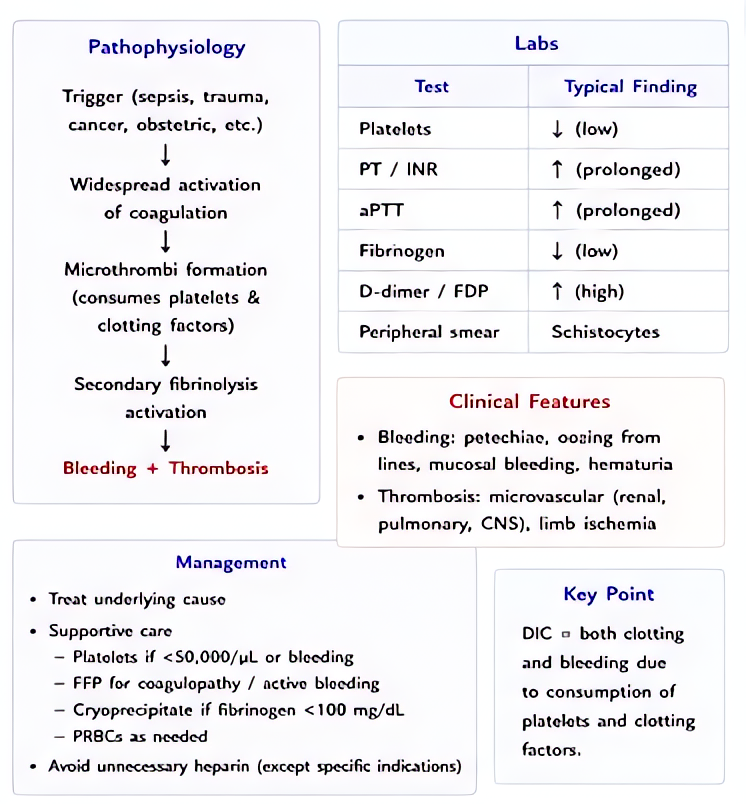
- ×Active intravascular clotting (DIC)
- ×Subarachnoid hemorrhage (relative — CRASH-3 mixed)
- ×History of seizure or QT prolongation (relative)
Clinical pearls
- ★Trauma: maximum benefit if given < 3 h post-injury; avoid > 3 h (mortality may worsen).
- ★Cardiac dosing varies widely — Mehta et al. recommend ≤ 50 mg/kg total for fewer seizures.
- ★Topical use (joint, surgical field) effective with minimal systemic exposure.
Other drugs in Coagulation Related
- Heparin (unfractionated)
Activates antithrombin → inactivates IIa (thrombin) and Xa.
- Protamine Sulfate
Strongly basic (positive-charge) protein binds to highly acidic (negative-charge) heparin → inactive ionic complex → renal excretion. 1 mg protamine neutralizes ~100 units heparin.
- DDAVP (Desmopressin)
Selective V2 agonist (renal water retention + Factor VIII/vWF release from endothelial Weibel-Palade bodies). NO V1 vasopressor activity at therapeutic dose.
- Warfarin
Inhibits vitamin K epoxide reductase (VKORC1) → depletes reduced vitamin K → ↓ synthesis of factors II, VII, IX, X and proteins C/S. Full effect takes days (waits for existing factor decay).
- Enoxaparin
Antithrombin-mediated inhibition, weighted toward factor Xa over IIa (~3.8:1). More predictable than UFH — no routine monitoring.
- Dalteparin
Antithrombin-mediated factor Xa > IIa inhibition. Similar profile to enoxaparin; preferred LMWH in cancer-associated VTE (CLOT trial).
- Tinzaparin
Antithrombin-mediated factor Xa > IIa inhibition; higher mean molecular weight than enoxaparin (anti-Xa:IIa ~1.9:1).
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert