Protamine Sulfate
Heparin antagonist
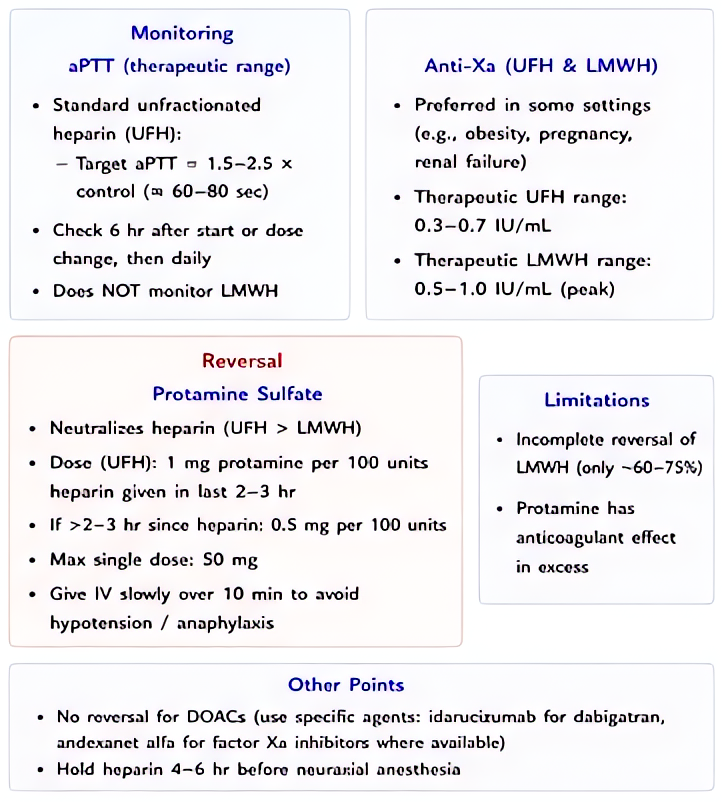
Strongly basic (positive-charge) protein binds to highly acidic (negative-charge) heparin → inactive ionic complex → renal excretion. 1 mg protamine neutralizes ~100 units heparin.
Indications
- •Reversal of unfractionated heparin post-CPB or vascular surgery
- •Partial reversal of LMWH (incomplete — neutralizes ~60% of enoxaparin anti-Xa activity)
- •Heparin overdose with active bleeding
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Post-CPB heparin reversal | 1 mg per 100 units heparin given (or use ACT-guided dose; usually 250-300 mg total for adult cardiac case) | — |
| Recent IV heparin (within 30 min) | 1 mg per 100 units heparin remaining | — |
| Subcutaneous heparin | Same calculation but slow infusion over 8-16 hr (ongoing absorption) | — |
| LMWH (enoxaparin) reversal | 1 mg per 1 mg enoxaparin if given <8h ago; partial reversal only | — |
Pharmacokinetics
Onset 1-5 min IV; duration of heparin neutralization ~2 hr; metabolized rapidly by plasma proteases.
Hemodynamic effects
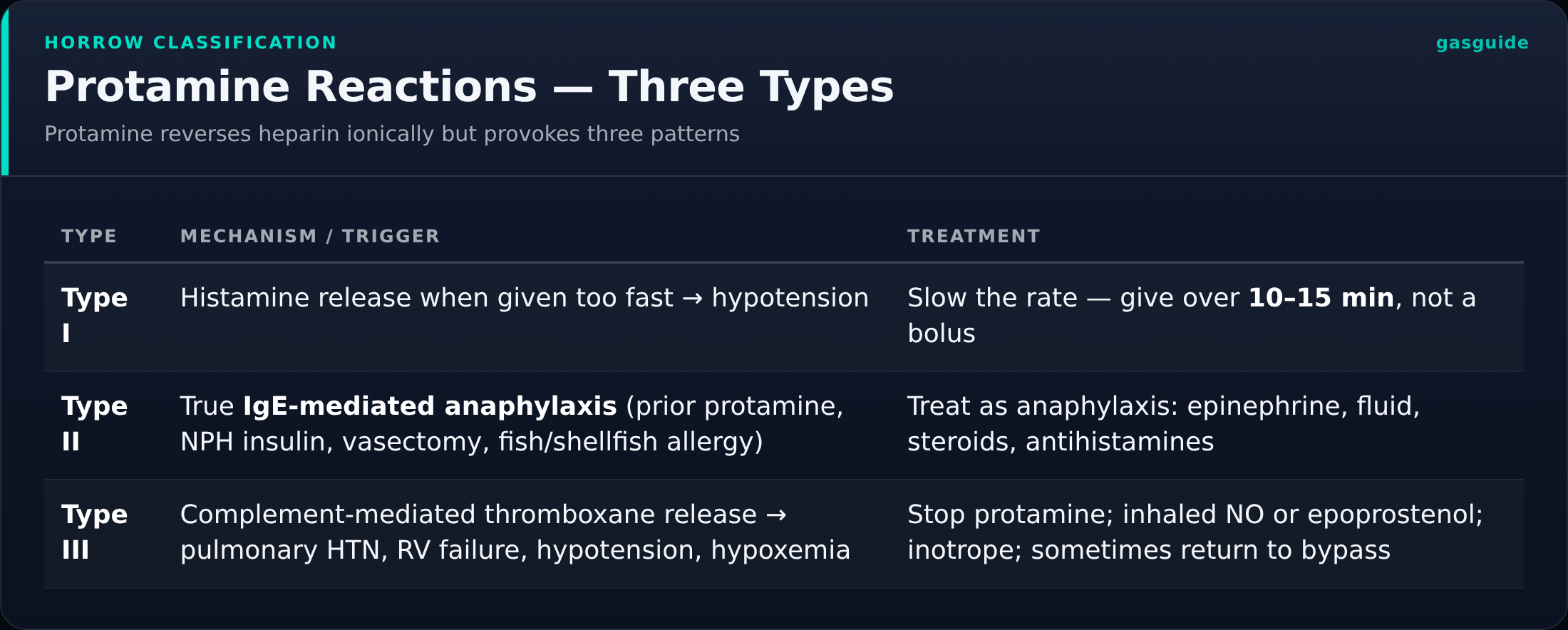
Slow IV (over 5-10 min) — rapid push causes histamine release → hypotension + flushing + bradycardia. Severe reactions (5-30 min after dose) include pulmonary hypertension + RV failure (catastrophic in cardiac surgery).
Side effects
- !Hypotension (dose-related, especially with rapid administration)
- !Pulmonary hypertension + RV failure (Type III reaction — life-threatening)
- !Anaphylaxis (Type II reaction — particularly in fish-allergy + prior protamine + diabetics on NPH insulin which contains protamine)
- !Bradycardia, flushing
- !Paradoxical anticoagulant effect at very high doses (>2× heparin dose)
Contraindications
- ×Prior anaphylaxis to protamine
- ×Caution: fish allergy (cross-reactivity), vasectomy patients (anti-protamine antibodies), patients on NPH insulin (cross-sensitivity, increased reaction risk)
Reversal / antidote
No specific antidote. Supportive: vasopressors, volume, possibly more heparin if pulmonary HTN crisis.
Clinical pearls
- ★POST-CPB CALCULATION: total heparin dose given (often 300-400 units/kg) → reverse with 1:100 ratio; verify with ACT (target return to baseline <130 sec). Most cardiac centers test then re-dose.
- ★REACTION TYPES: I — hypotension from rapid push (slow infusion next time); II — anaphylactic IgE; III — pulmonary HTN + RV failure (catastrophic, often fatal — can develop minutes after apparently uneventful dose).
- ★FISH ALLERGY mythology: actual cross-reactivity rate is LOW. Document allergy + slow administration + premedicate (steroid, H1, H2 blocker) — but don't withhold if needed.
- ★DON'T overdose: protamine at >2× heparin dose has its own anticoagulant effect (binds platelet factors). Aim for exact neutralization.
Other drugs in Coagulation Related
- Heparin (unfractionated)
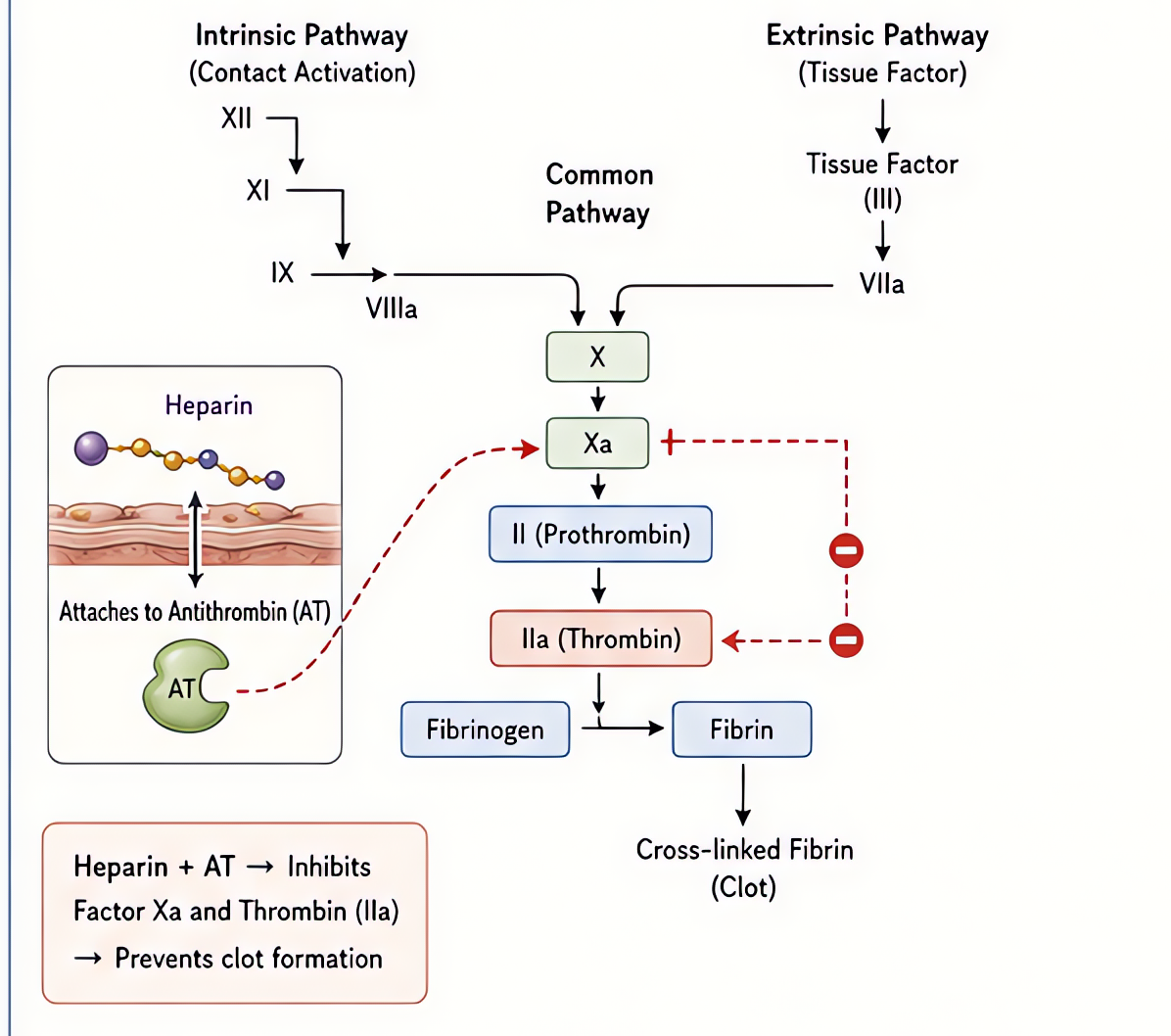
Activates antithrombin → inactivates IIa (thrombin) and Xa.
- Tranexamic Acid (TXA)
Reversibly binds plasminogen, blocking conversion to plasmin → preserves fibrin clot.
- DDAVP (Desmopressin)
Selective V2 agonist (renal water retention + Factor VIII/vWF release from endothelial Weibel-Palade bodies). NO V1 vasopressor activity at therapeutic dose.
- Warfarin
Inhibits vitamin K epoxide reductase (VKORC1) → depletes reduced vitamin K → ↓ synthesis of factors II, VII, IX, X and proteins C/S. Full effect takes days (waits for existing factor decay).
- Enoxaparin
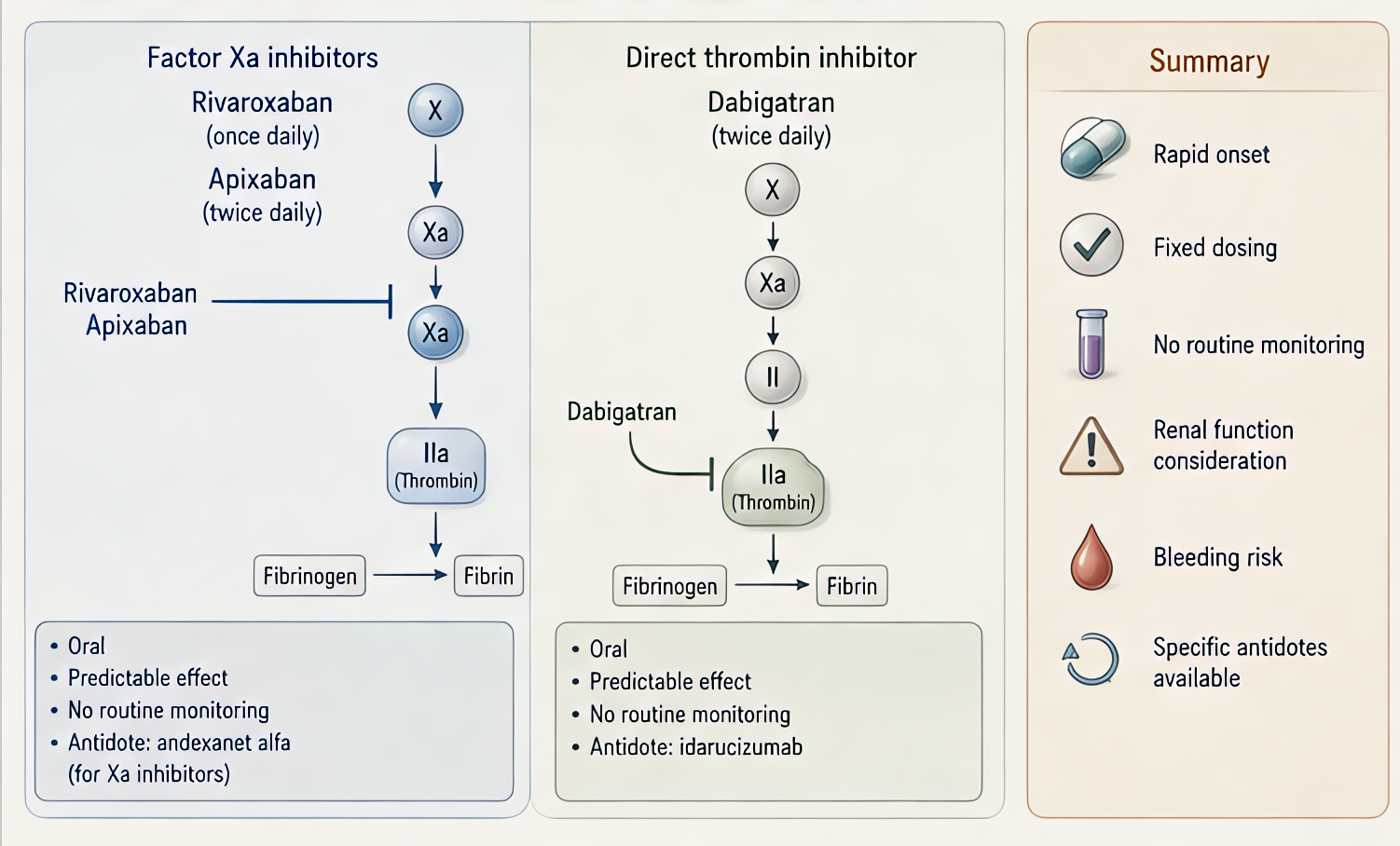
Antithrombin-mediated inhibition, weighted toward factor Xa over IIa (~3.8:1). More predictable than UFH — no routine monitoring.
- Dalteparin
Antithrombin-mediated factor Xa > IIa inhibition. Similar profile to enoxaparin; preferred LMWH in cancer-associated VTE (CLOT trial).
- Tinzaparin
Antithrombin-mediated factor Xa > IIa inhibition; higher mean molecular weight than enoxaparin (anti-Xa:IIa ~1.9:1).
- Fondaparinux
Binds antithrombin → selective, exclusive factor Xa inhibition (no IIa activity). Does NOT cause HIT — safe alternative in HIT patients.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert