Packed Red Blood Cells (PRBC)
pRBC · Leukoreduced RBC
Concentrated allogeneic erythrocytes for transfusion
Volume of concentrated red cells (Hct 55–80%) suspended in additive solution (AS-1, AS-3, AS-5). Restores oxygen-carrying capacity and transiently expands intravascular volume. One unit ≈ 300 mL.
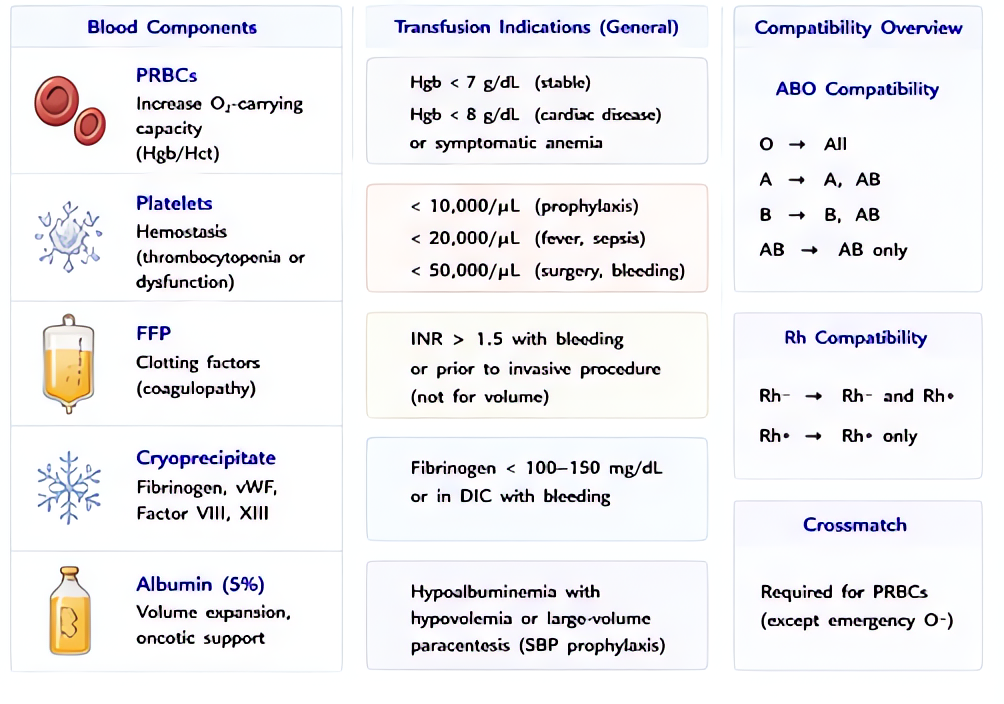
Indications
- •Acute hemorrhage with hemodynamic instability or signs of inadequate oxygen delivery
- •Hb <7 g/dL in stable hospitalized non-cardiac patients (TRICC, TRISS)
- •Hb <8 g/dL in cardiac surgery, symptomatic CAD, or active ACS
- •Symptomatic anemia (chest pain, dyspnea, orthostasis, lactic acidosis) regardless of trigger threshold
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Adult unit | 1 unit (≈300 mL) raises Hb ≈1 g/dL and Hct ≈3% in a 70 kg adult | — |
| Pediatric / neonatal | 10–15 mL/kg over 2–4 h (4 mL/kg raises Hb ≈1 g/dL) | |
| Massive transfusion protocol | 1:1:1 ratio with FFP and platelets (PROPPR 2015) — typically 6 PRBC : 6 FFP : 1 apheresis-platelet pack | — |
Pharmacokinetics
Stored 42 days in AS-1/AS-3 at 1–6 °C. 24-h post-transfusion survival 75–90% (AABB target). Senescent transfused cells removed by reticuloendothelial system over weeks.
Hemodynamic effects
300 mL volume → ↑preload, ↑BP. Calcium-citrate binding can drop ionized Ca²⁺ with rapid massive transfusion (>1 unit per 5 min) → hypotension.
Respiratory effects
TRALI risk — non-cardiogenic pulmonary edema within 6 h. TACO risk — volume overload, especially in CHF and elderly.
Side effects
- !Acute hemolytic transfusion reaction (ABO incompatibility) — fever, chills, hypotension, hemoglobinuria, DIC; STOP transfusion immediately
- !Febrile non-hemolytic transfusion reaction (cytokines from donor leukocytes; mitigated by leukoreduction)
- !Transfusion-related acute lung injury (TRALI) — leading cause of transfusion-related mortality in the US
- !Transfusion-associated circulatory overload (TACO)
- !Allergic / anaphylactic (anti-IgA in IgA-deficient patient)
- !Transfusion-transmitted infection (HCV 1:1.6M, HIV 1:1.5M, HBV 1:300K, bacterial contamination ~1:5000 platelets, much rarer for RBC)
- !Hyperkalemia from old units in renal failure / massive pediatric transfusion
- !Hypocalcemia (citrate)
- !Citrate toxicity → metabolic alkalosis after the citrate is metabolized
Contraindications
- ×Acute hemolytic reaction in progress
- ×Religious refusal (Jehovah's Witness — alternative bloodless protocols)
- ×ABO/Rh incompatibility without emergency type-O override
Clinical pearls
- ★TRICC (NEJM 1999) + TRISS (NEJM 2014): restrictive (Hb 7) non-inferior to liberal (Hb 9–10) in stable critical illness. Liberal not better — and often worse for ICU mortality.
- ★EMERGENCY RELEASE: O-negative for women of childbearing age, O-positive otherwise. Type-specific available in 5–10 min if patient blood is sent stat. Crossmatched in 30–60 min.
- ★MASSIVE TRANSFUSION 1:1:1: PROPPR (JAMA 2015) showed 1:1:1 reduced 24-h hemorrhagic death vs 1:1:2; activate MTP early when 4+ units anticipated in 1 h.
- ★OLD UNITS (>21 d) DEBATE: ABLE (NEJM 2015) and TRANSFUSE (NEJM 2017) showed no outcome difference between fresh and standard-issue units — practice can use whatever's available except in select situations (intrauterine, large-volume neonatal).
- ★TRALI MITIGATION: male-only or never-pregnant-female plasma reduces TRALI risk — modern blood banks select these donors for plasma and platelets.
Other drugs in Blood Products
- Fresh Frozen Plasma (FFP)
Plasma frozen within 8 h (FFP) or 24 h (FFP24/PF24) of collection. Contains all coagulation factors at near-physiologic concentrations (~1 unit/mL of each factor, plus ~400 mg fibrinogen per unit). Volume per unit ≈ 250 mL.
- Platelets (Apheresis or Pooled)
Single-donor apheresis unit (~3–4×10¹¹ platelets in ~250 mL) or pooled whole-blood-derived (5–6 random donor units; equivalent platelet count). Restores primary hemostasis.
- Cryoprecipitate
Cold-insoluble fraction of FFP. Each ~15-mL unit contains ≥150 mg fibrinogen, ~80 IU factor VIII, ~40–70% of donor vWF, factor XIII, and fibronectin. Most concentrated source of fibrinogen.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •AABB Circular of Information for the Use of Human Blood and Blood Components