Platelets (Apheresis or Pooled)
Apheresis platelets · Random-donor pooled platelets
Platelet concentrate for transfusion
Single-donor apheresis unit (~3–4×10¹¹ platelets in ~250 mL) or pooled whole-blood-derived (5–6 random donor units; equivalent platelet count). Restores primary hemostasis.
Indications
- •Bleeding with platelet count <50K (or <100K for CNS, ophthalmologic, neuraxial procedures)
- •Prophylaxis at platelet count <10K in stable thrombocytopenia (PLADO trial)
- •Prophylaxis <20K with fever, sepsis, anticoagulation, or imminent invasive procedure
- •Functional platelet defect (uremia, antiplatelet drug, congenital) with active bleeding
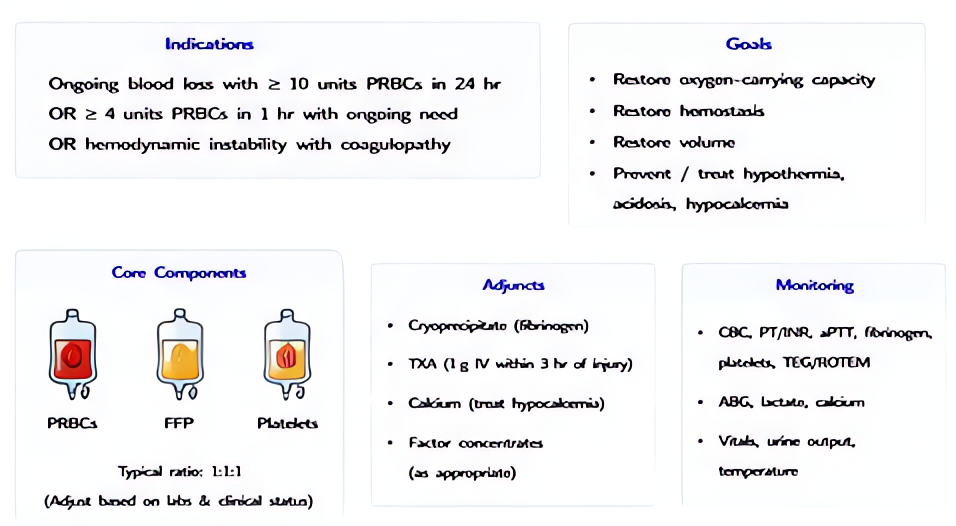
- •Massive transfusion 1:1:1 protocol
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Adult | 1 apheresis unit OR 5–6 pooled random-donor units; raises platelet count by 30–60K | |
| Pediatric | 5–10 mL/kg raises platelet count by 50–100K | |
| Massive transfusion ratio | 1 apheresis unit for every 6 units PRBC (PROPPR 1:1:1) | — |
Pharmacokinetics
Stored 5 days at 20–24 °C with continuous gentle agitation. Half-life 3–4 days in non-immune recipient; minutes-to-hours in HIT, ITP, splenic sequestration, or active bleeding.
Hemodynamic effects
250 mL volume; minor hemodynamic effect.
Respiratory effects
TRALI risk — historically the highest of any blood product per unit because plasma volume is high and stored at warm temp; mitigated by male-donor / pathogen-reduction.
Side effects
- !Bacterial contamination — highest of any blood product (~1:2000–1:5000) because of room-temperature storage; pathogen-reduced products reduce this risk substantially
- !Febrile non-hemolytic reaction (very common — leukocytes in product)
- !Allergic / urticarial
- !TRALI
- !Alloimmunization to HLA antigens → platelet refractoriness (give HLA-matched if confirmed)
- !Rh sensitization (Rh+ platelet to Rh− woman of childbearing age — give Rh-immunoglobulin)
Contraindications
- ×TTP (worsens microthrombosis — exception: life-threatening bleed)
- ×HIT (worsens thrombosis — exception: life-threatening bleed)
- ×Heparin-induced thrombocytopenia, post-transfusion purpura
Clinical pearls
- ★REFRACTORINESS: a 1-h post-transfusion increment <7,500/μL on two consecutive transfusions = platelet refractoriness. Send HLA antibody screen; switch to HLA-matched.
- ★ABO MATCHING: identical-ABO platelets give a higher count rise than non-identical, but ABO mismatch is acceptable in an emergency. Volume-load matters in pediatrics.
- ★NEURAXIAL THRESHOLD: ASRA recommends platelets >80K (some institutions 75–100K) for spinal/epidural placement. Higher threshold for catheter REMOVAL than placement.
- ★ITP PARADOX: in idiopathic thrombocytopenic purpura, transfused platelets are consumed within hours. Reserve for active bleeding; use IVIG, steroids, or TPO agonist for count support.
- ★POST-TRANSFUSION PURPURA: severe thrombocytopenia 5–10 d post-transfusion in HPA-1a-negative patient — IVIG 1 g/kg × 2 days is treatment of choice; platelet transfusion paradoxically worsens.
Other drugs in Blood Products
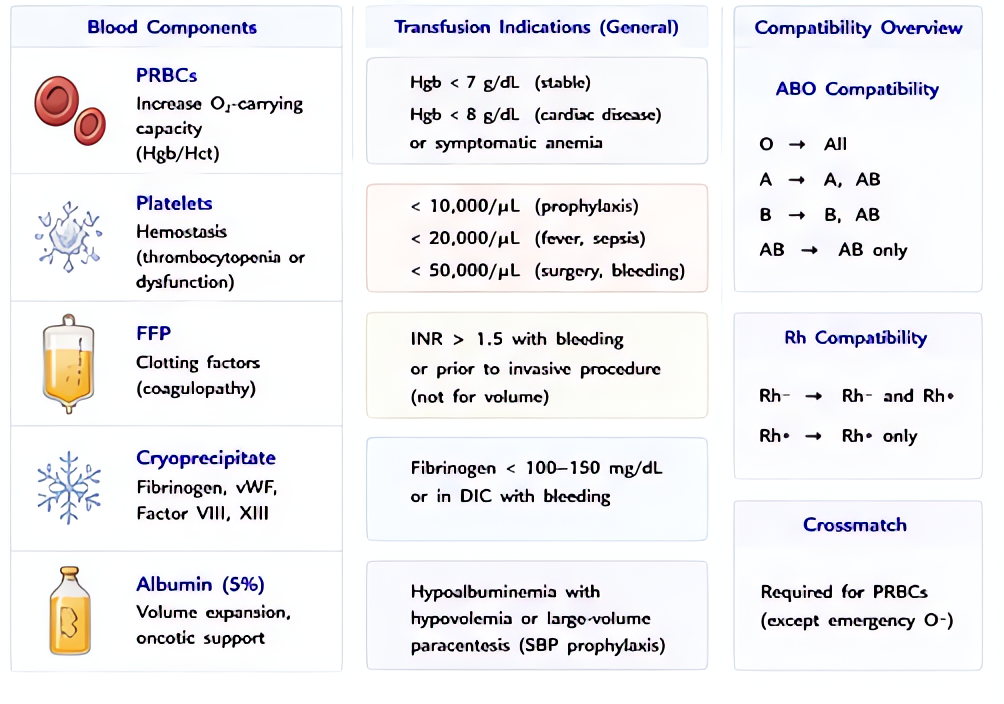
- Packed Red Blood Cells (PRBC)
Volume of concentrated red cells (Hct 55–80%) suspended in additive solution (AS-1, AS-3, AS-5). Restores oxygen-carrying capacity and transiently expands intravascular volume. One unit ≈ 300 mL.
- Fresh Frozen Plasma (FFP)
Plasma frozen within 8 h (FFP) or 24 h (FFP24/PF24) of collection. Contains all coagulation factors at near-physiologic concentrations (~1 unit/mL of each factor, plus ~400 mg fibrinogen per unit). Volume per unit ≈ 250 mL.
- Cryoprecipitate
Cold-insoluble fraction of FFP. Each ~15-mL unit contains ≥150 mg fibrinogen, ~80 IU factor VIII, ~40–70% of donor vWF, factor XIII, and fibronectin. Most concentrated source of fibrinogen.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •AABB Circular of Information for the Use of Human Blood and Blood Components