Insulin (Regular / Humulin R)
Humulin R · Novolin R
Short-acting human insulin
Binds insulin receptors → tyrosine kinase cascade → GLUT4 translocation in muscle/fat (glucose uptake), glycogen + lipid synthesis, K+ shift intracellularly.
Indications
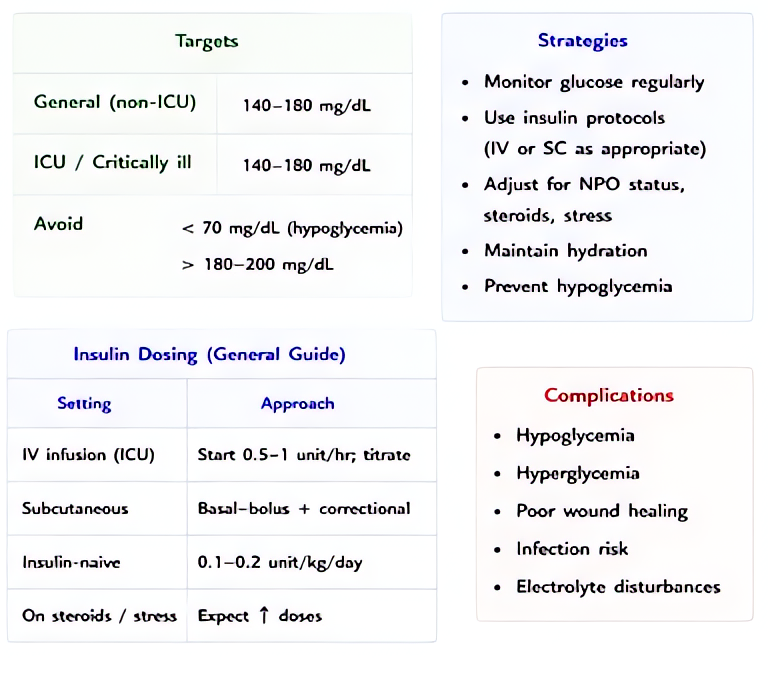
- •Intraoperative hyperglycemia management (T1DM, T2DM, stress-induced)
- •DKA / HHS
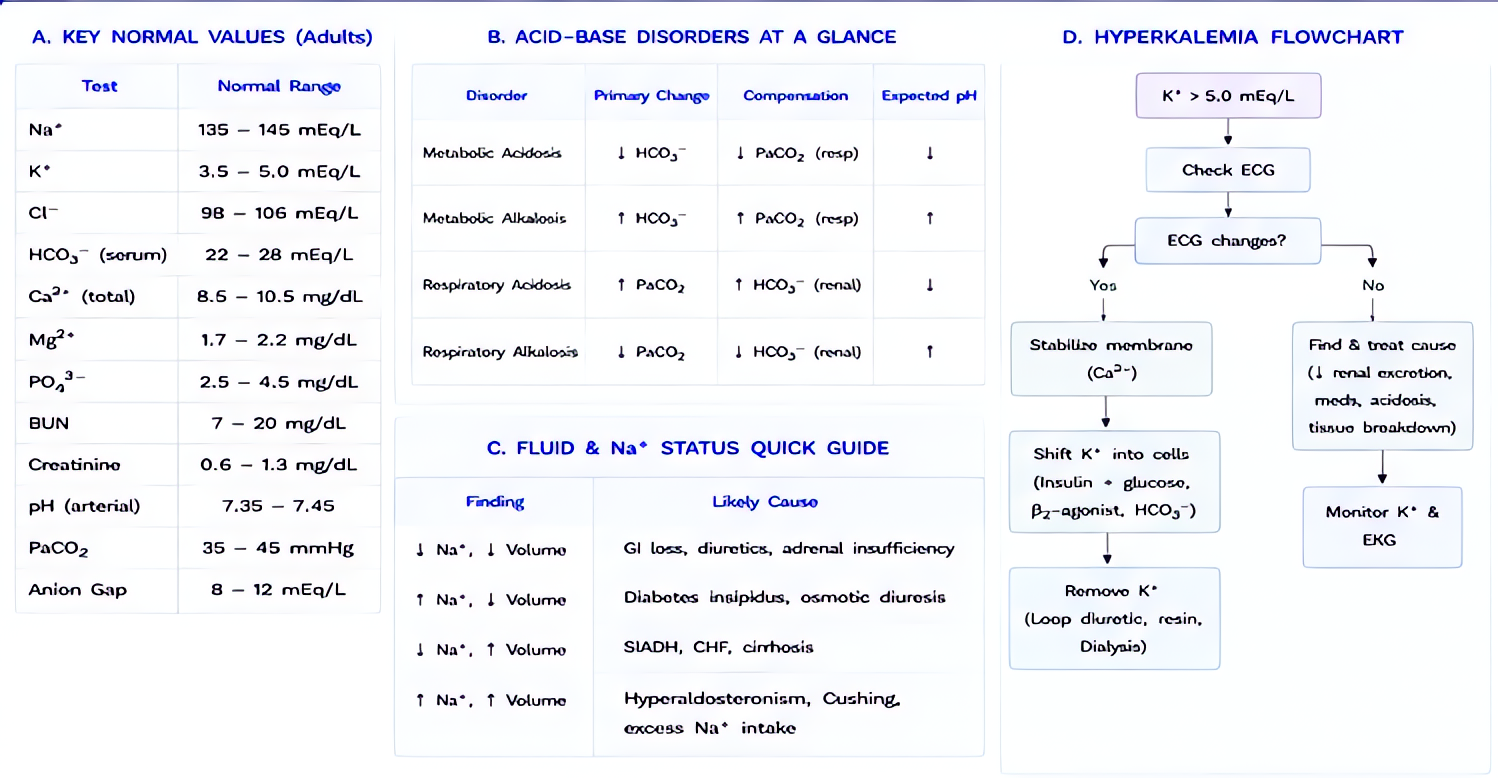
- •Hyperkalemia (with dextrose to avoid hypoglycemia)
- •Beta-blocker / calcium-channel-blocker overdose (high-dose insulin euglycemia therapy)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Intraop sliding scale (BG 180–250) | 2–4 U IV bolus | — |
| Intraop infusion (BG > 250) | 0.05–0.1 U/kg/h IV, titrate to BG 140–180 | — |
| DKA | 0.1 U/kg/h IV (no bolus needed per ADA 2024) | — |
| Hyperkalemia | 10 U IV with 25 g dextrose (1 amp D50) | — |
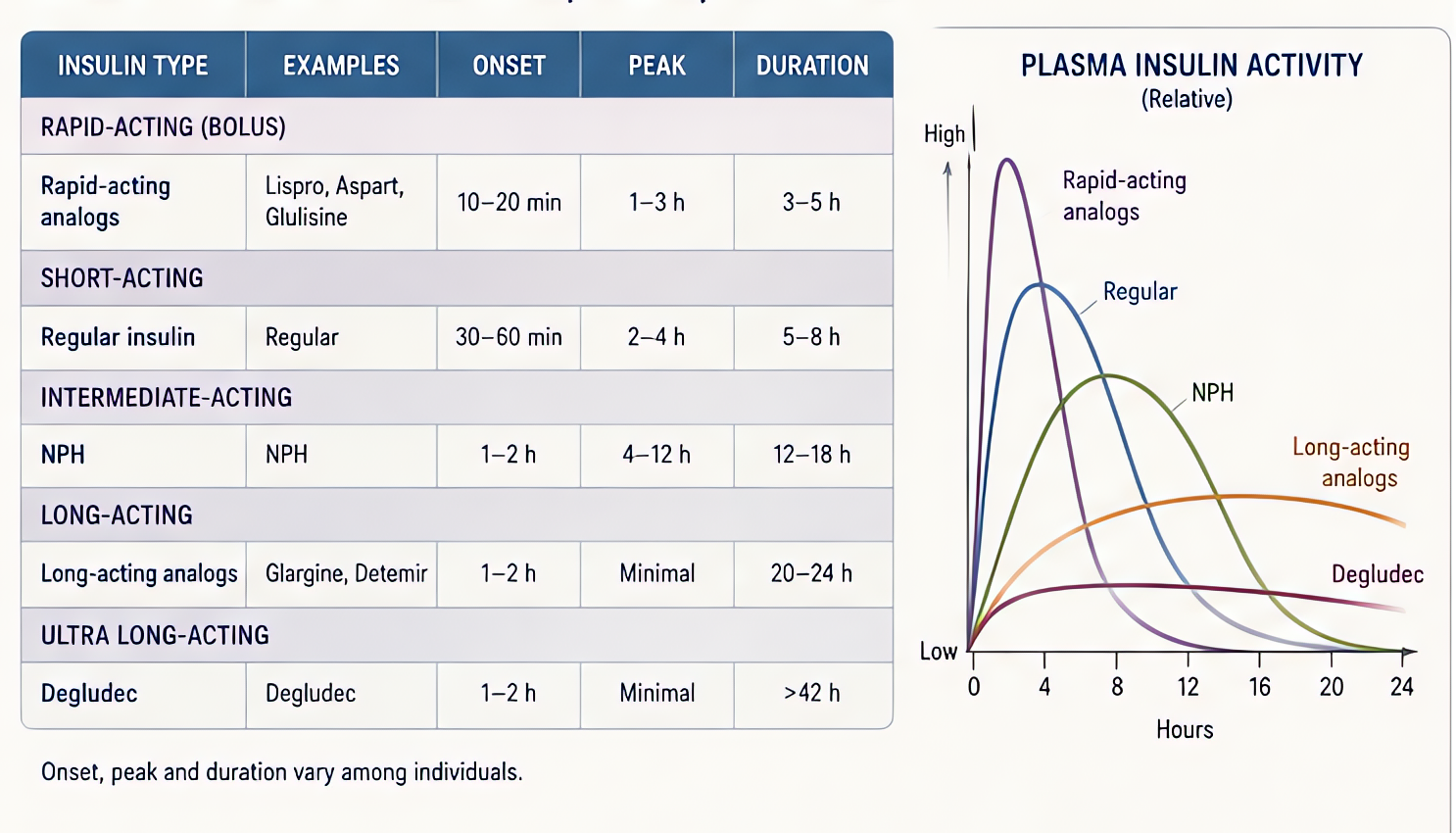
Pharmacokinetics
IV onset immediate, peak 30 min, duration 2–4 h. SC onset 30 min, peak 2–4 h, duration 6–8 h. Hepatic + renal degradation.
Hemodynamic effects
Indirect — hypoglycemia → tachycardia, hypertension, then hypotension if severe.
Respiratory effects
None directly.
Side effects
- !Hypoglycemia (the universal risk — must monitor BG q30 min during infusion)
- !Hypokalemia (intracellular shift)
- !Allergic reactions (rare with human insulin)
- !Lipodystrophy at SC sites (chronic)
Contraindications
- ×Hypoglycemia
- ×Hypokalemia (relative — must replace K+ first if < 3.3 in DKA)
Clinical pearls
- ★INTRAOP TARGET: 140–180 mg/dL per most cardiac/critical-care guidelines. Tighter (80–110) increases hypoglycemia risk without mortality benefit (NICE-SUGAR).
- ★HYPERKALEMIA: 10 U regular insulin + 25 g dextrose drops K+ by 0.5–1 mEq/L within 30 min. Expect rebound — repeat or move to dialysis.
- ★DKA POTASSIUM RULE: K+ < 3.3 → hold insulin, replace K+ first. K+ 3.3–5.3 → start insulin + add 20–30 mEq KCl/L. K+ > 5.3 → insulin without K+ replacement.
- ★STORAGE: regular insulin is the only IV-compatible insulin — analogues (lispro, aspart) are SC only at standard concentrations.
- ★ABSORPTION TO IV TUBING: insulin binds plastic. Flush IV line with 20 mL of insulin-containing fluid before starting infusion or first 30 min is sub-dosed.
Other drugs in Sugar Control
- Glucagon
Binds Gs-coupled glucagon receptors → ↑cAMP → activates phosphorylase, drives glycogenolysis + gluconeogenesis. In cardiac tissue, the cAMP rise produces inotropic + chronotropic effects independent of β-receptors.
- Dextrose 50% (D50)
Concentrated glucose (50 g per 100 mL = 25 g per 50 mL amp/syringe). Direct serum glucose elevation by passive distribution; insulin-independent immediate availability to brain.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert