Glucagon
GlucaGen
Pancreatic α-cell hormone analogue
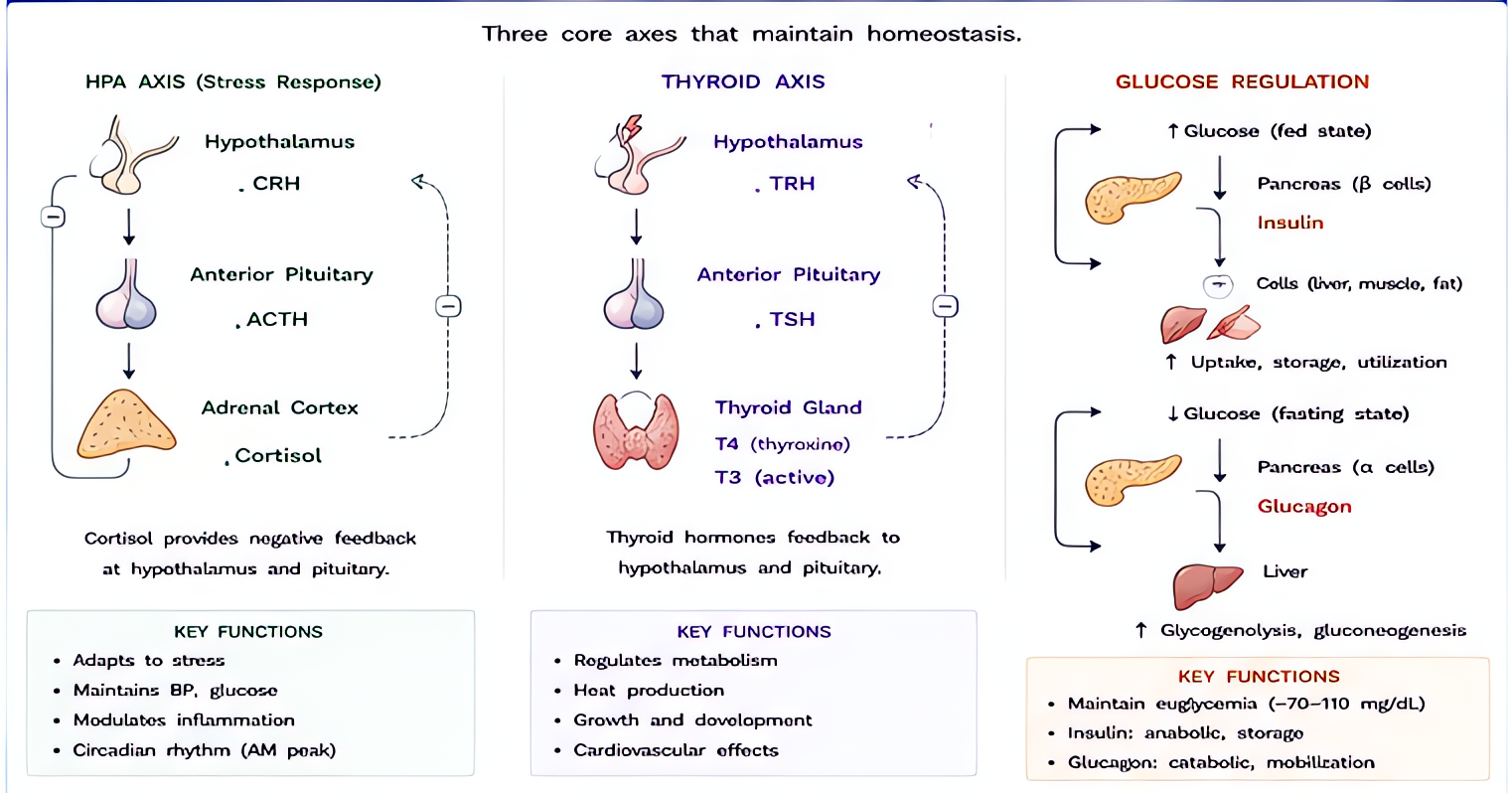
Binds Gs-coupled glucagon receptors → ↑cAMP → activates phosphorylase, drives glycogenolysis + gluconeogenesis. In cardiac tissue, the cAMP rise produces inotropic + chronotropic effects independent of β-receptors.
Indications
- •Severe hypoglycemia without IV access (community / pre-hospital)
- •Beta-blocker overdose (refractory bradycardia + hypotension despite atropine + epi)
- •Calcium channel blocker overdose (adjunct to high-dose insulin + calcium)
- •Esophageal foreign-body / spasm relaxation (smooth-muscle)
- •Diagnostic: GI motility studies
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Hypoglycemia | 1 mg IM/SC/IV | 0.5 mg if < 25 kg, 1 mg if ≥ 25 kg |
| β-blocker overdose | 5–10 mg IV bolus, then 1–10 mg/h infusion | — |
| GI smooth-muscle relaxation | 0.5–1 mg IV | — |
Pharmacokinetics
Onset 1 min IV / 5–15 min IM. Duration 30 min (hypoglycemia reversal — short, then food/dextrose needed). Hepatic + renal degradation.
Hemodynamic effects
Positive inotropy + chronotropy (HR + 20–30 bpm, BP + 10–15 mmHg) at high overdose-treatment doses. Mild effect at hypoglycemia dose.
Respiratory effects
None directly.
Side effects
- !Nausea + vomiting (most common; severe at overdose doses — pretreat with ondansetron)
- !Hyperglycemia
- !Hypokalemia
- !Tachycardia, palpitations
- !Allergic reactions (rare)
Contraindications
- ×Pheochromocytoma (causes catecholamine release)
- ×Insulinoma (paradoxical hypoglycemia rebound)
- ×Glycogen-depleted states (alcoholic patients, prolonged fasting — won't work; give dextrose instead)
Clinical pearls
- ★β-BLOCKER OVERDOSE: glucagon bypasses β-receptor — works when atropine + epi don't. Pretreat with ondansetron because the high-dose nausea is bad.
- ★GLYCOGEN-DEPLETED PATIENTS: glucagon needs hepatic glycogen to work. Alcoholics, anorexics, prolonged-NPO patients won't respond — give D50 instead.
- ★HYPOGLYCEMIA REBOUND: 30-min duration means the patient WILL re-drop. Always follow with food or dextrose infusion.
- ★PREGNANCY: doesn't cross placenta meaningfully — safe in pregnant diabetics with severe hypoglycemia.
Other drugs in Sugar Control
- Insulin (Regular / Humulin R)
Binds insulin receptors → tyrosine kinase cascade → GLUT4 translocation in muscle/fat (glucose uptake), glycogen + lipid synthesis, K+ shift intracellularly.
- Dextrose 50% (D50)
Concentrated glucose (50 g per 100 mL = 25 g per 50 mL amp/syringe). Direct serum glucose elevation by passive distribution; insulin-independent immediate availability to brain.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert