Methylprednisolone
Solu-Medrol · Medrol
Intermediate-acting synthetic glucocorticoid
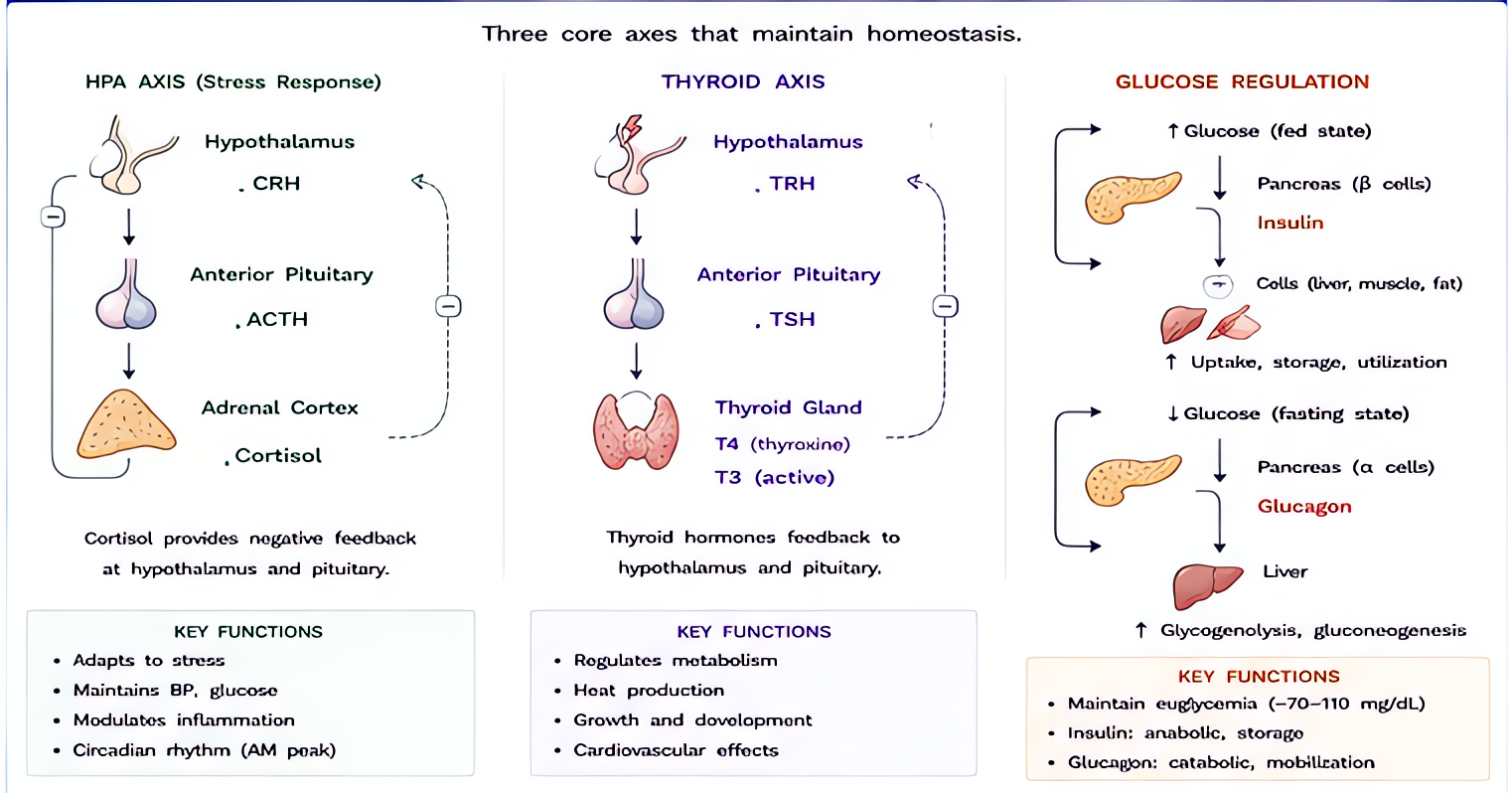
Binds intracellular glucocorticoid receptor → translocation to nucleus → transcriptional regulation of anti-inflammatory genes (lipocortin-1, IL-10) + suppression of pro-inflammatory genes (NF-κB, COX-2). 5× the glucocorticoid potency of hydrocortisone with minimal mineralocorticoid activity.
Indications
- •Acute asthma / COPD exacerbation
- •Anaphylaxis adjunct (after epinephrine + antihistamines)
- •Severe allergic / contrast reactions
- •Organ-transplant induction immunosuppression
- •Airway edema (post-extubation stridor, croup)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Anaphylaxis / severe allergy | 125 mg IV; repeat q6 h × 24 h | — |
| Asthma exacerbation | 40–125 mg IV q6 h | — |
| Post-extubation stridor prophylaxis | 20 mg IV q4 h × 4 doses (Cheng et al, Crit Care 2006) | — |
Pharmacokinetics
IV onset 1 h. Peak 4–8 h. Biological half-life 12–36 h. Hepatic metabolism + renal excretion.
Hemodynamic effects
Mineralocorticoid effect minimal — no salt retention or hypertension at usual doses.
Respiratory effects
Reduces airway inflammation; clinical effect 4–6 h post-dose.
Side effects
- !Hyperglycemia (especially diabetic patients)
- !Hypertension (high-dose, prolonged)
- !Adrenal suppression (>3 weeks of therapy)
- !Infection susceptibility
- !Wound healing impairment
- !Avascular necrosis of femoral head (high-dose)
- !Mood changes / steroid psychosis (high-dose)
Contraindications
- ×Untreated systemic fungal infection
- ×Live vaccine within 4 weeks
- ×Hypersensitivity
Clinical pearls
- ★NASCIS PROTOCOLS WITHDRAWN AT MOST CENTERS: high-dose methylprednisolone in acute spinal cord injury showed marginal motor benefit at the cost of more sepsis, GI bleeds, pneumonia. Cochrane and current AANS/CNS guidelines no longer recommend.
- ★POST-EXTUBATION STRIDOR (CRIT CARE 2006, FRANÇOIS): in ICU patients with positive cuff-leak test, 20 mg q4 h × 4 doses pre-extubation reduced stridor and reintubation. Standard at most large centers.
- ★DOSE EQUIVALENCE: 4 mg methylprednisolone = 5 mg prednisolone = 20 mg hydrocortisone = 0.75 mg dexamethasone (glucocorticoid effect).
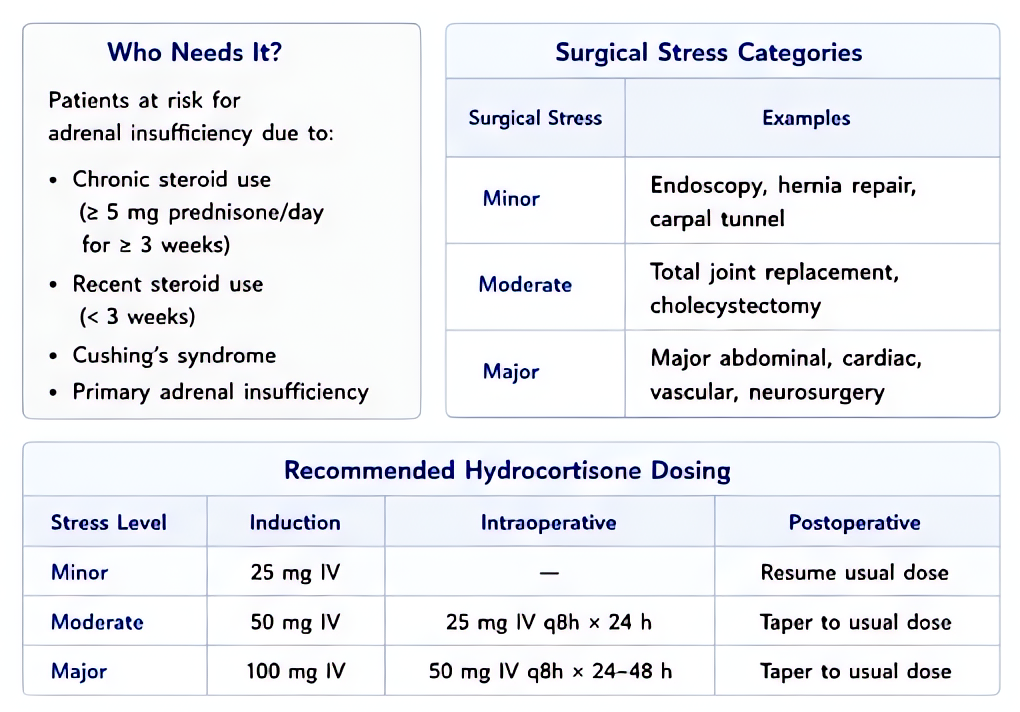
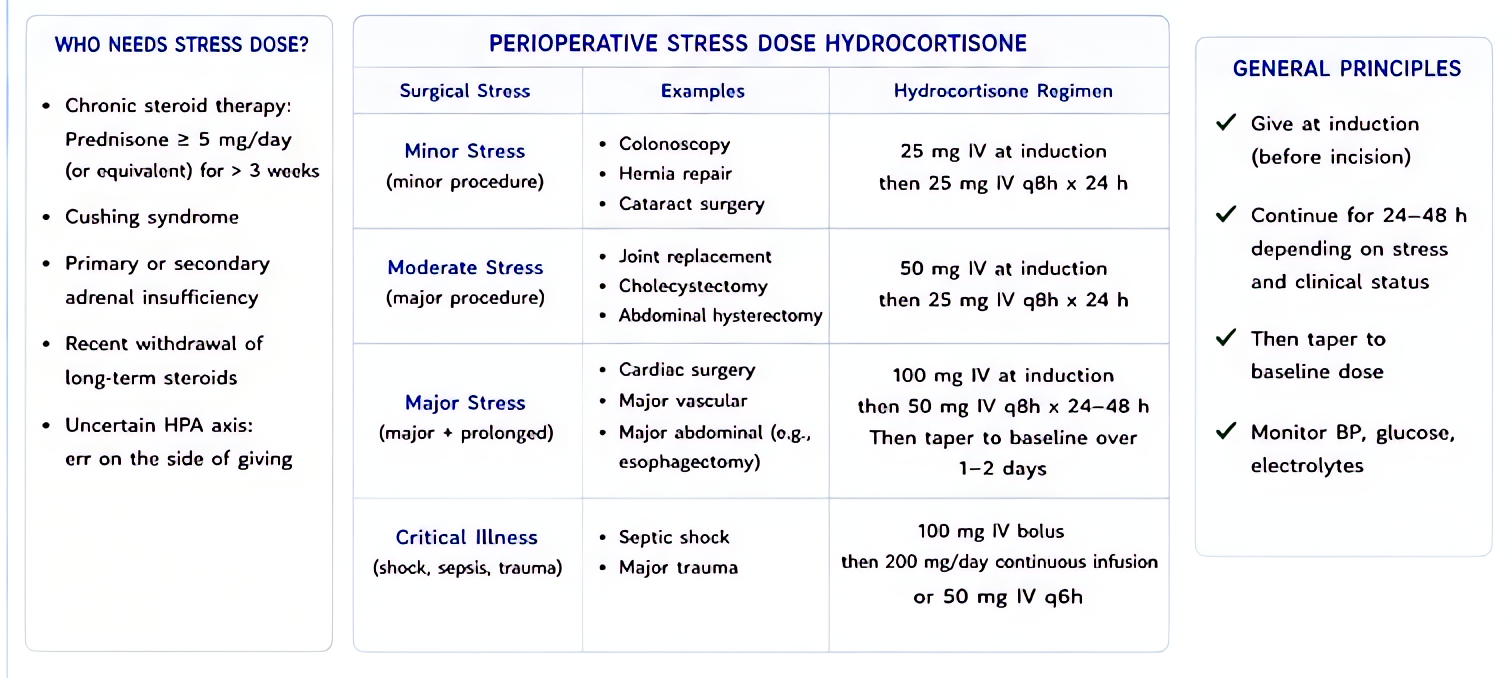
- ★STRESS-DOSE STEROIDS: not methylprednisolone's role — hydrocortisone covers both glucocorticoid AND mineralocorticoid (which methylprednisolone doesn't).
Other drugs in Steroids
- Dexamethasone
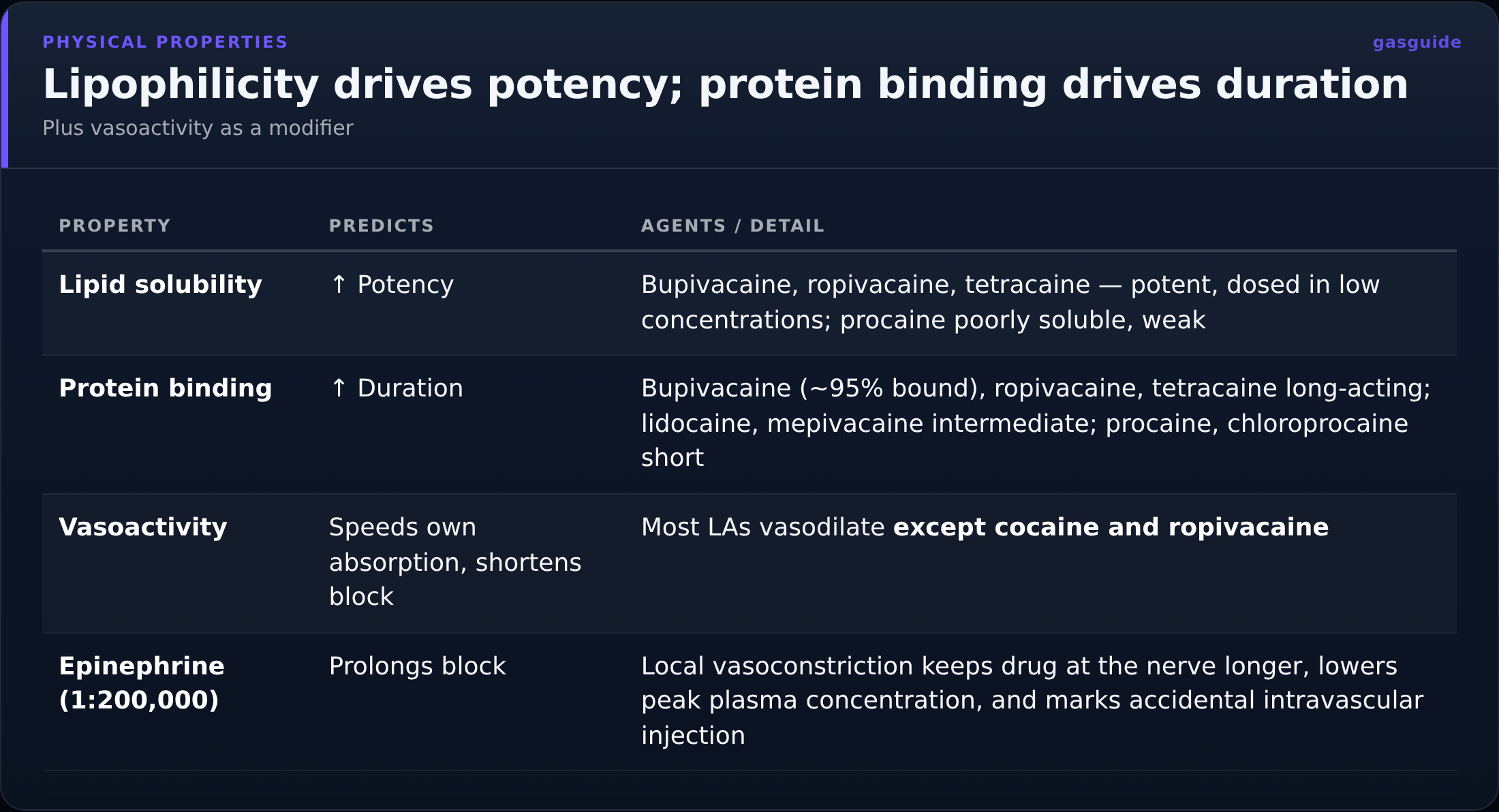
Glucocorticoid receptor agonist — anti-inflammatory, antiemetic, prolongs PNB duration.
- Hydrocortisone
Endogenous cortisol equivalent. Binds both glucocorticoid AND mineralocorticoid receptors — 1× glucocorticoid potency (reference standard), substantial mineralocorticoid effect (sodium retention, K⁺ excretion). The replacement steroid for adrenal insufficiency.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert