Hydrocortisone
Solu-Cortef · Cortef
Short-acting glucocorticoid + mineralocorticoid
Endogenous cortisol equivalent. Binds both glucocorticoid AND mineralocorticoid receptors — 1× glucocorticoid potency (reference standard), substantial mineralocorticoid effect (sodium retention, K⁺ excretion). The replacement steroid for adrenal insufficiency.
Indications
- •Acute adrenal crisis (Addisonian crisis)
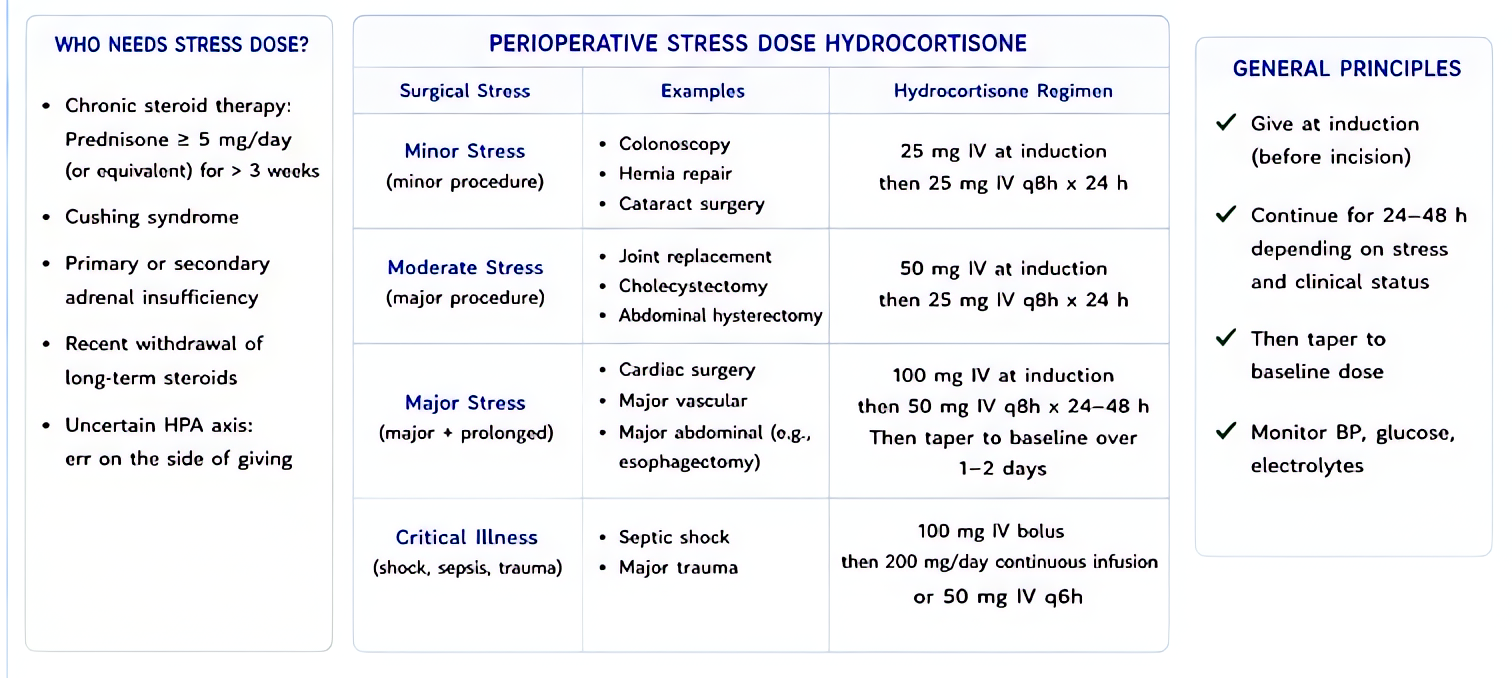
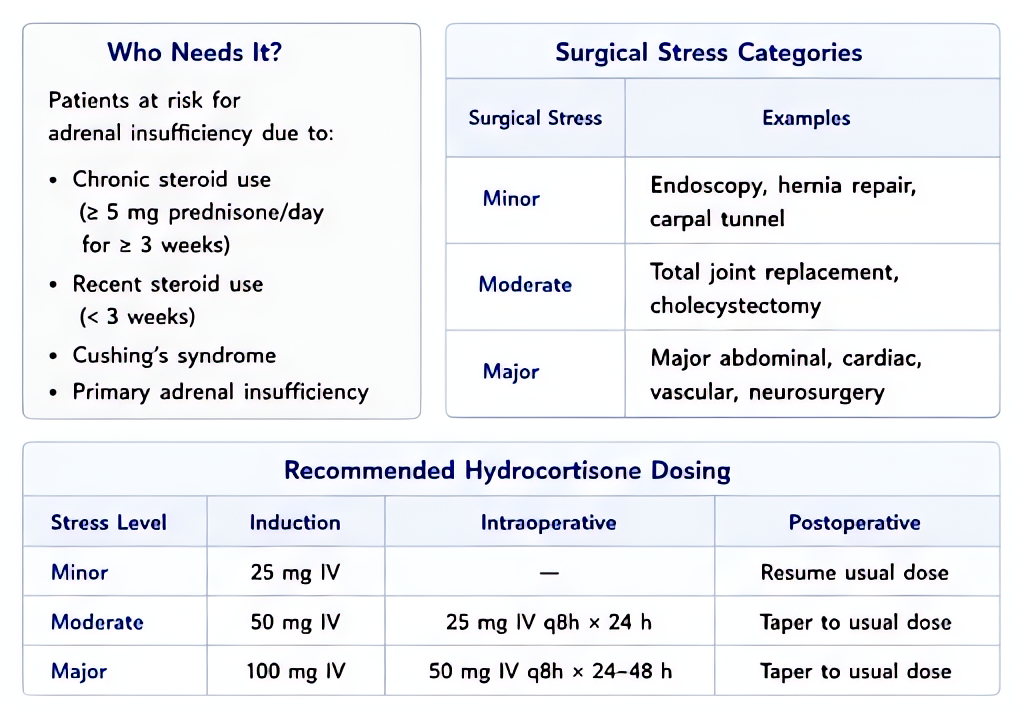
- •Stress-dose perioperative coverage in patients on chronic steroids or with adrenal insufficiency
- •Septic shock with vasopressor-refractory hypotension (Surviving Sepsis 2021 conditional)
- •Anaphylaxis adjunct
- •Adrenal insufficiency replacement (PO maintenance)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Adrenal crisis | 100 mg IV bolus, then 50 mg IV q6 h for 24 h, taper | — |
| Stress-dose major surgery | 100 mg IV at induction, then 50 mg IV q8 h × 24–48 h | — |
| Septic shock | 200 mg/day IV continuous infusion or 50 mg q6 h until vasopressors weaned | — |
| Maintenance replacement | 15–25 mg/day PO divided | — |
Pharmacokinetics
Onset minutes IV (free cortisol acts directly). Peak 30 min. Biological half-life 8–12 h. Hepatic metabolism.
Hemodynamic effects
Mineralocorticoid effect → sodium and water retention, mild blood pressure support — useful in shock states.
Respiratory effects
Reduces airway inflammation; secondary effect.
Side effects
- !Hyperglycemia
- !Sodium / water retention, hypertension
- !Hypokalemia (mineralocorticoid)
- !Adrenal suppression with chronic use
- !Infection susceptibility
Contraindications
- ×Untreated systemic fungal infection
- ×Hypersensitivity
Clinical pearls
- ★STRESS-DOSE LOGIC: chronic steroid users (>5 mg prednisone-equivalent for >3 weeks within last year) cannot mount the cortisol surge that surgery requires. Cover with hydrocortisone per the major-vs-minor scheme. Failure → vasopressor-refractory hypotension during/after induction.
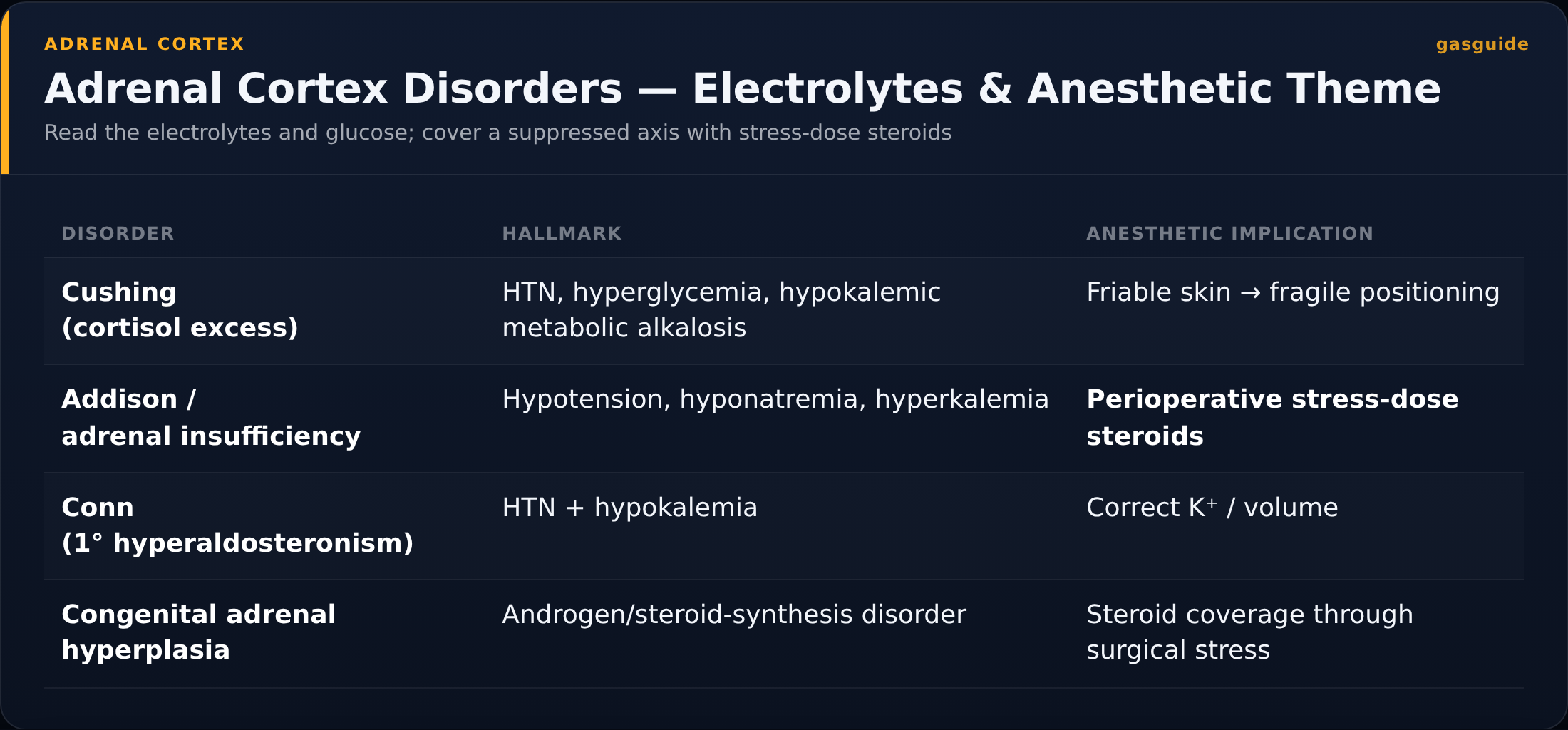
- ★ADRENAL CRISIS: hypotension + nausea + abdominal pain + hypoglycemia + hyperkalemia + hyponatremia in a patient with adrenal disease history. 100 mg IV stat saves lives.
- ★SEPTIC SHOCK (SURVIVING SEPSIS 2021): 200 mg/day for vasopressor-refractory hypotension. ADRENAL trial (NEJM 2018) showed faster shock reversal; APROCCHSS showed mortality benefit.
- ★REPLACEMENT VS STRESS: don't confuse. Maintenance is 15–25 mg/day. Stress dosing for major surgery is 100–300 mg/day for 24–48 h.
Other drugs in Steroids
- Dexamethasone
Glucocorticoid receptor agonist — anti-inflammatory, antiemetic, prolongs PNB duration.
- Methylprednisolone
Binds intracellular glucocorticoid receptor → translocation to nucleus → transcriptional regulation of anti-inflammatory genes (lipocortin-1, IL-10) + suppression of pro-inflammatory genes (NF-κB, COX-2). 5× the glucocorticoid potency of hydrocortisone with minimal mineralocorticoid activity.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert