Hydroxyethyl Starch (HES) — generally avoided in 2026
Hespan (6% HES 670/0.75) · Voluven (6% HES 130/0.4)
Synthetic colloid — modified amylopectin
Polymer of hydroxyethylated glucose units derived from waxy maize. Provides oncotic volume expansion similar to albumin. Higher-molecular-weight / higher-substitution products (Hespan) cause more renal dysfunction than lower-substitution products (Voluven), but both have been shown harmful in critical illness.
Indications
- •Mostly historical / largely abandoned in CRNA practice as of FDA boxed warning (2013, expanded 2021)
- •Limited cardiac surgery use in some institutions (off-CPB volume expansion) — local protocols vary
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Historical volume resuscitation | Up to 50 mL/kg/day (Voluven 6% HES 130/0.4) — but FDA-warned not for use in critical illness | — |
Pharmacokinetics
Half-life depends on molecular weight + substitution; smaller particles excreted in urine, larger ones broken down by amylase over weeks. Persistent tissue deposition in skin (pruritus), liver, kidney.
Hemodynamic effects
1:1 to 1.4:1 volume expansion versus infused — similar to albumin.
Respiratory effects
TRALI not described, but pulmonary edema from over-resuscitation possible.
Side effects
- !Acute kidney injury / need for renal replacement therapy (CHEST, 6S NEJM 2012) — INCREASED in critical illness vs crystalloid
- !Coagulopathy — interferes with vWF, platelet function, factor VIII
- !Persistent pruritus from cutaneous deposition
- !Anaphylactoid reactions
- !Hyperamylasemia (amylase complexes with HES)
- !Excess mortality at 90 days in sepsis (6S Trial)
Contraindications
- ×Critical illness, sepsis, severe liver disease (FDA boxed warning 2013, 2021)
- ×Pre-existing renal dysfunction or RRT
- ×Coagulopathy or active bleeding (worsens it)
- ×ICU patients
- ×Cardiac surgery in patients with renal risk factors
Clinical pearls
- ★FDA BOXED WARNING (2013, expanded 2021): do NOT use HES in critically ill patients including sepsis. Real-world use has dropped >80% in US ICUs since.
- ★6S TRIAL (NEJM 2012, Perner): in severe sepsis, HES 130/0.4 vs Ringer's acetate — HES had higher 90-day mortality (51% vs 43%, p=0.03) and more renal replacement therapy. This trial ended HES in sepsis.
- ★CHEST TRIAL (NEJM 2012, Myburgh): HES 130/0.4 vs saline in 7000 ICU patients — no mortality difference but more RRT (7.0% vs 5.8%) and adverse events with HES.
- ★WHEN CRYSTALLOID + ALBUMIN ARE OPTIONS, USE THEM. HES has no clinical scenario where it outperforms a balanced crystalloid + judicious albumin in modern practice.
- ★AANA / ASA POSITION: most institutions have removed HES from formulary or restricted to specific cardiac-surgery use cases with informed consent. CRNAs should not be initiating HES outside of an explicit local protocol.
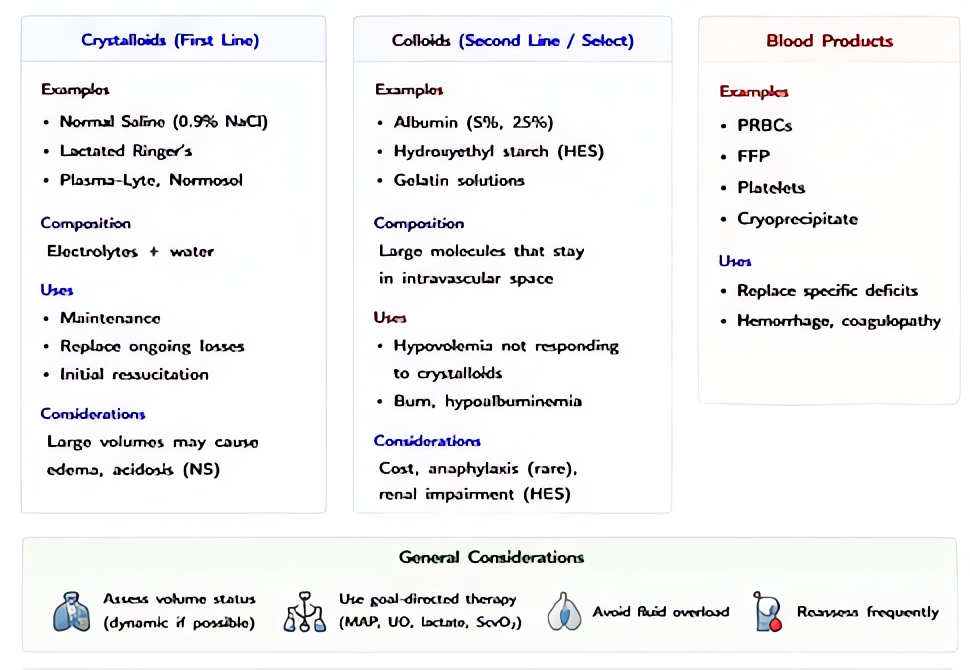
Other drugs in Colloids
- Albumin 5% (iso-oncotic)
Heat-treated, pasteurized human serum albumin in 0.9% NaCl at 5% concentration. Iso-oncotic with normal plasma — expands intravascular volume approximately 1:1 with infused volume by maintaining colloid oncotic pressure.
- Albumin 25% (hyper-oncotic)
5× more concentrated than 5% albumin. Hyper-oncotic — pulls interstitial fluid into the intravascular space. 100 mL of 25% albumin can expand plasma volume by 400–500 mL by drawing fluid across the capillary membrane.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert