Albumin 5% (iso-oncotic)
Albuminar 5% · Plasbumin 5%
Iso-oncotic human serum albumin colloid
Heat-treated, pasteurized human serum albumin in 0.9% NaCl at 5% concentration. Iso-oncotic with normal plasma — expands intravascular volume approximately 1:1 with infused volume by maintaining colloid oncotic pressure.
Indications
- •Volume resuscitation in hypotension (alternative to crystalloid when crystalloid resistance or large volumes are concerning)
- •Therapeutic plasmapheresis replacement fluid
- •Hepatorenal syndrome (with terlipressin or norepinephrine)
- •Spontaneous bacterial peritonitis (1.5 g/kg day 1, 1 g/kg day 3)
- •Large-volume paracentesis (8 g albumin per L of ascites removed when >5 L)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Volume resuscitation | 250–500 mL IV; titrate to hemodynamic endpoint | — |
| Hepatorenal syndrome | 1 g/kg IV day 1 (max 100 g), then 25–50 g/day with terlipressin or norepinephrine | — |
| Large-volume paracentesis | 8 g per L removed beyond 5 L | — |
Pharmacokinetics
Intravascular half-life 16 h in healthy patients; shorter in capillary leak (sepsis, burn). Heat-pasteurized (60 °C × 10 h) — no transmission of HCV/HIV/HBV.
Hemodynamic effects
1:1 volume expansion. Slower onset than crystalloid bolus but more sustained intravascular retention.
Respiratory effects
Pulmonary edema possible if cardiac dysfunction + over-resuscitation.
Side effects
- !Allergic / anaphylactoid reactions (rare)
- !Volume overload
- !Hypotension during rapid infusion (rare)
- !No transmissible-infection risk (heat-pasteurized) — long-standing safety advantage over plasma products
Contraindications
- ×Severe anemia or cardiac failure where volume cannot be tolerated
- ×Hypersensitivity
Clinical pearls
- ★SAFE TRIAL (NEJM 2004): in 7000 ICU patients, 4% albumin and 0.9% saline produced equivalent 28-day mortality. Albumin not superior in general ICU population — but cost considerations have made crystalloid the default.
- ★ALBIOS TRIAL (NEJM 2014): in severe sepsis, albumin to target ≥30 g/L did NOT reduce 28- or 90-day mortality but improved hemodynamics. Reasonable in volume-refractory shock; not standard.
- ★TBI EXCLUSION: SAFE post-hoc analysis showed worse outcomes with albumin in TBI — saline is the volume of choice in head trauma.
- ★CIRRHOSIS USES: SBP, hepatorenal syndrome, large-volume paracentesis — these are the indications where albumin has clear mortality benefit (not generic 'low albumin' replacement, which doesn't help).
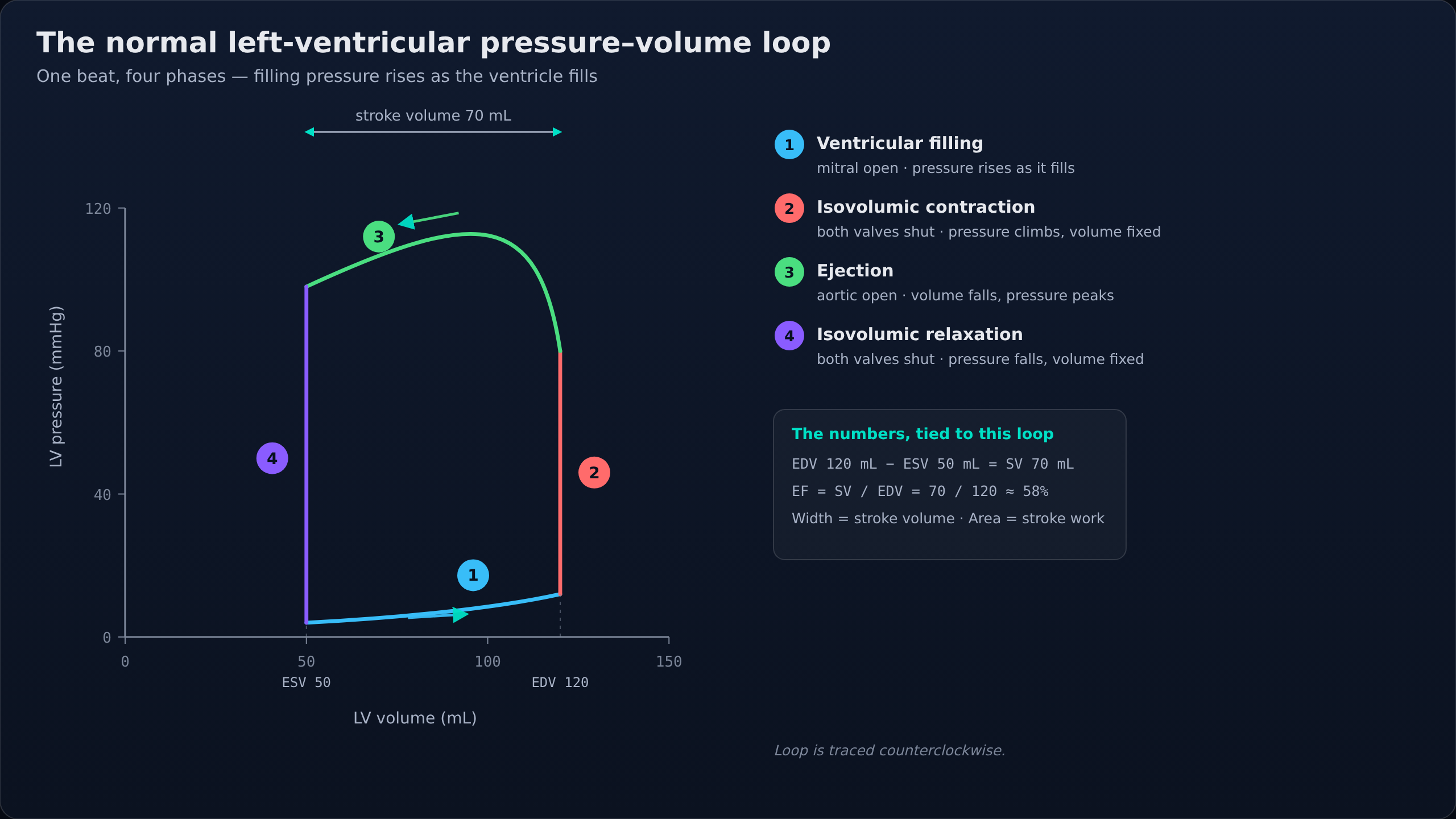
- ★VOLUME EXPANSION ESTIMATE: 100 mL of 5% albumin pulls roughly 100 mL of fluid INTO the intravascular space — a 1:1 effective volume expander, smaller volume than the 3:1 crystalloid equivalent.
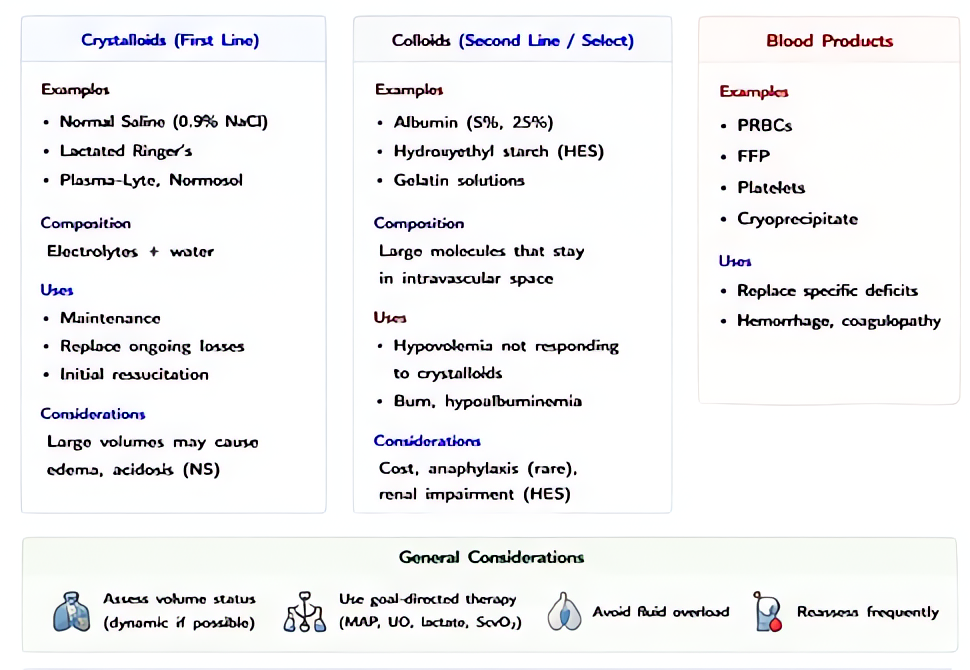
Other drugs in Colloids
- Albumin 25% (hyper-oncotic)
5× more concentrated than 5% albumin. Hyper-oncotic — pulls interstitial fluid into the intravascular space. 100 mL of 25% albumin can expand plasma volume by 400–500 mL by drawing fluid across the capillary membrane.
- Hydroxyethyl Starch (HES) — generally avoided in 2026
Polymer of hydroxyethylated glucose units derived from waxy maize. Provides oncotic volume expansion similar to albumin. Higher-molecular-weight / higher-substitution products (Hespan) cause more renal dysfunction than lower-substitution products (Voluven), but both have been shown harmful in critical illness.
Browse all classes: /reference/drugs
Suggested reading
- •Miller's Anesthesia, 9e
- •FDA package insert