Pyridostigmine
Mestinon
Quaternary acetylcholinesterase inhibitor
Reversibly inhibits acetylcholinesterase → ↑acetylcholine at the neuromuscular junction. Quaternary ammonium → does NOT cross BBB → no CNS effects. Longer-acting than neostigmine; mainstay of chronic myasthenia gravis treatment.
Indications
- •Myasthenia gravis maintenance therapy (oral)
- •Reversal of non-depolarizing NMB (rare; neostigmine almost always preferred)
- •Reversal of antimuscarinic poisoning (alternative to physostigmine)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Myasthenia maintenance | 60 mg PO q4–6 h, titrated to clinical response (max 1500 mg/day) | — |
| Reversal of NMB (rare) | 0.1–0.25 mg/kg IV with glycopyrrolate | — |
Pharmacokinetics
PO peak 1–2 h. Half-life 3–4 h (twice neostigmine's). Renal excretion ~80%.
Hemodynamic effects
Muscarinic effects → bradycardia, hypotension if not blocked with anticholinergic.
Respiratory effects
Bronchospasm + secretions if unopposed by glycopyrrolate.
Side effects
- !Cholinergic crisis with overdose (excess weakness, salivation, bronchorrhea, bradycardia)
- !GI cramping, diarrhea (most common; dose-limiting in chronic use)
- !Bradycardia
- !Bronchospasm
Contraindications
- ×Mechanical GI/urinary obstruction
- ×Hypersensitivity
Clinical pearls
- ★MYASTHENIA PERIOPERATIVE: continue pyridostigmine on the day of surgery; missing a dose can precipitate myasthenic crisis. Be prepared for both excess (cholinergic crisis if overdosed) and deficit (myasthenic crisis if doses missed) — ICE pack to eyelid distinguishes them at bedside.
- ★MYASTHENIA + NMB DOSE: pyridostigmine reduces sensitivity to non-depolarizers (sugammadex preferred for reversal — bypasses the receptor entirely). Use lower rocuronium doses; titrate with TOF.
- ★EDROPHONIUM TENSILON TEST: historical pyridostigmine adjunct to confirm myasthenia. Largely abandoned for AChR antibody testing.
- ★CHOLINERGIC CRISIS RECOGNITION: muscle fasciculations + abdominal cramping + bronchorrhea on top of weakness = too much pyridostigmine. Treat with atropine, hold anticholinesterase, support ventilation.
Other drugs in Anticholinesterases
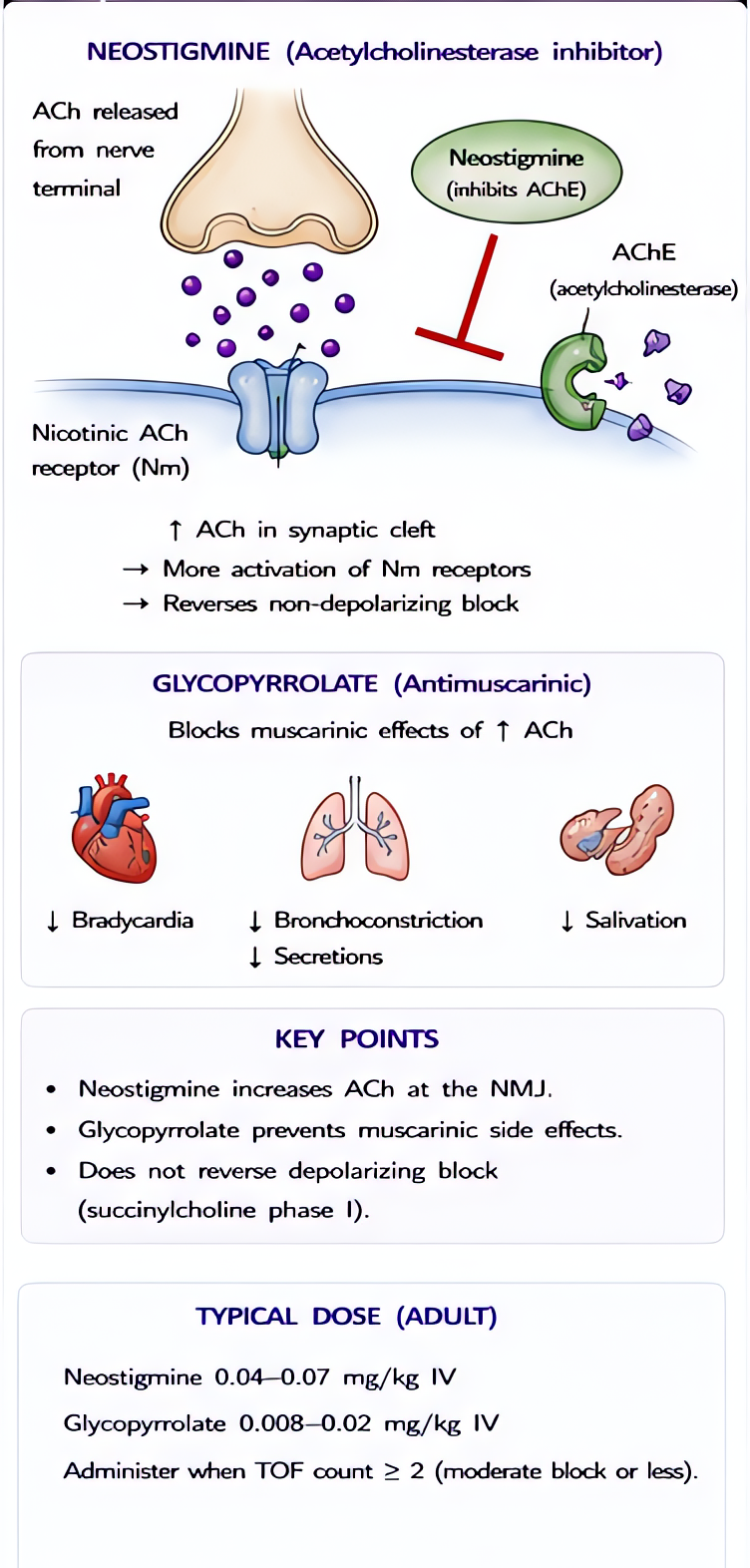
- Neostigmine
Reversibly inhibits AChE → ↑ACh at NMJ → outcompetes non-depolarizing relaxants. Co-administer antimuscarinic (glycopyrrolate or atropine) to block muscarinic side effects.
- Edrophonium
Reversible AChE inhibitor with the FASTEST onset (1–2 min) and SHORTEST duration (5–10 min) of the anticholinesterases. Quaternary structure → no CNS penetration. Largely historical; replaced by sugammadex in NMB reversal and by serologic AChR antibody testing in myasthenia diagnosis.
- Physostigmine
Reversible AChE inhibitor with TERTIARY amine structure → CROSSES blood-brain barrier (unlike neostigmine, pyridostigmine, edrophonium). The only AChE inhibitor that treats CENTRAL anticholinergic syndrome.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert