Physostigmine
Antilirium
Tertiary-amine acetylcholinesterase inhibitor (CNS-active)
Reversible AChE inhibitor with TERTIARY amine structure → CROSSES blood-brain barrier (unlike neostigmine, pyridostigmine, edrophonium). The only AChE inhibitor that treats CENTRAL anticholinergic syndrome.
Indications
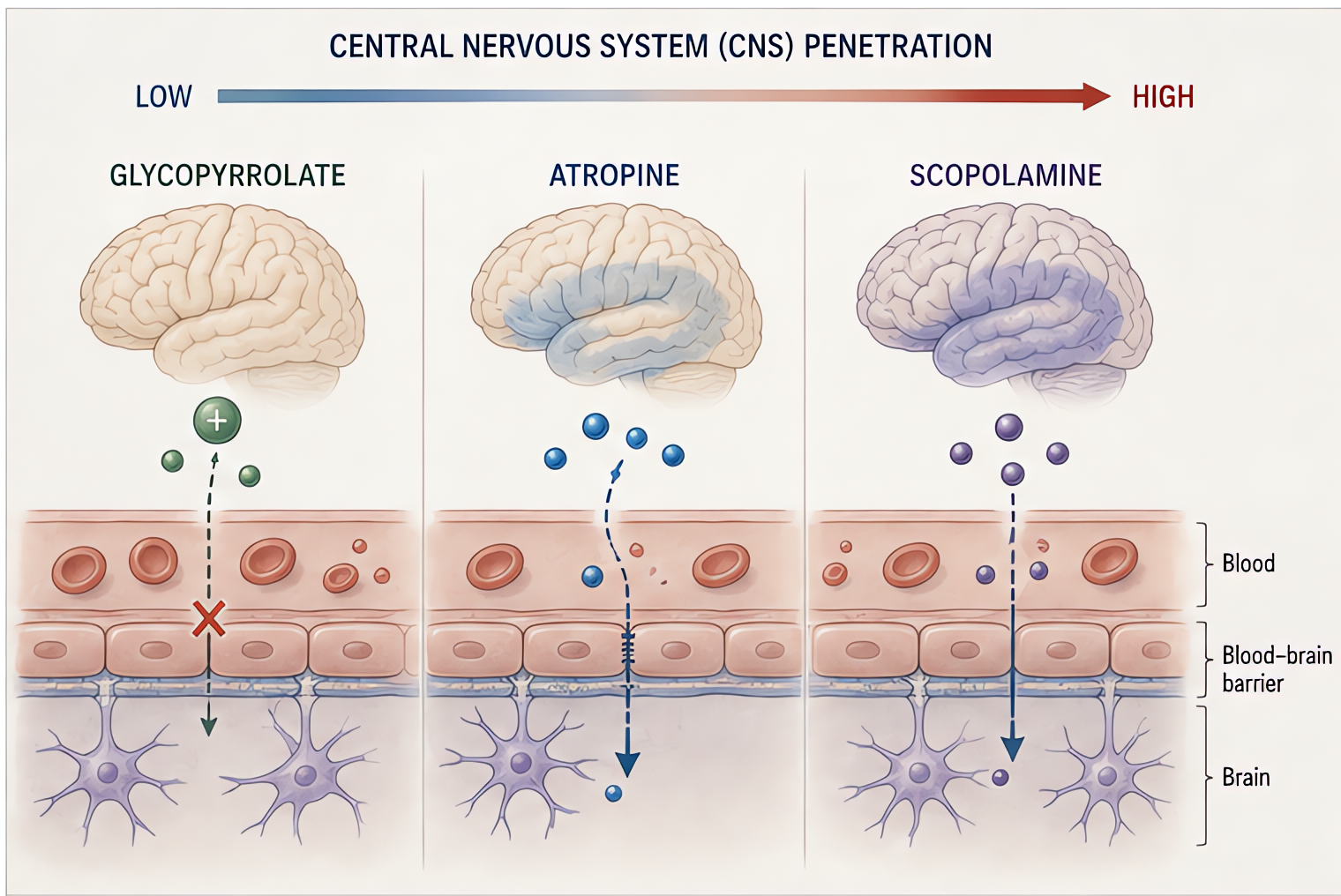
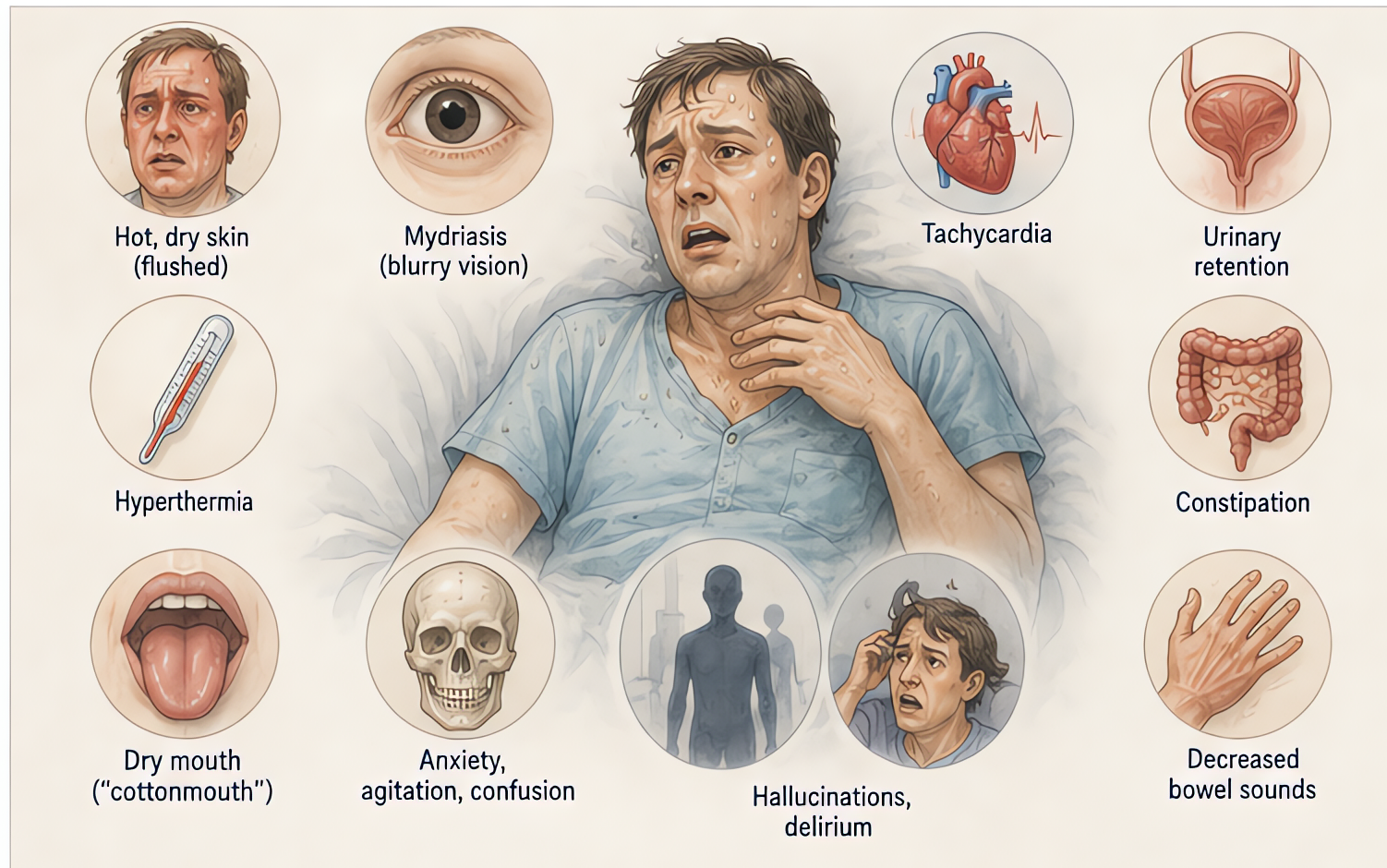
- •Central anticholinergic syndrome (atropine, scopolamine, jimson weed, antihistamine, TCA poisoning)
- •Postoperative delirium with suspected anticholinergic etiology
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Central anticholinergic syndrome | 1–2 mg IV slow over 5 min; repeat q10–30 min as needed | 0.02 mg/kg slow IV (max 0.5 mg/dose) |
Pharmacokinetics
Onset 3–8 min IV. Duration 30–60 min. Hepatic + plasma cholinesterase metabolism.
Hemodynamic effects
Bradycardia (atropine should be available before giving).
Respiratory effects
Bronchospasm + secretions at high dose.
Side effects
- !Cholinergic crisis at high dose (sweating, salivation, lacrimation, urination, defecation, GI cramps, emesis — SLUDGE)
- !Seizures (paradoxical CNS effect at high dose)
- !Bradycardia, asystole on rapid push
- !Bronchospasm
Contraindications
- ×Tricyclic antidepressant overdose with QRS widening (case reports of asystole — most authorities now permit cautious use, but check institutional protocols)
- ×Mechanical GI/GU obstruction
- ×Asthma (relative)
Clinical pearls
- ★THE BBB ONE: physostigmine is the ONLY AChE inhibitor that crosses BBB — the only one that reverses CENTRAL anticholinergic syndrome (delirium from scopolamine patches, anticholinergic overdose, post-op confusion in elderly).
- ★TCA OVERDOSE WARNING (HISTORICAL): a 1980s case series associated physostigmine with asystole in TCA toxicity; this concern has softened with modern data. Many toxicologists now use physostigmine cautiously even in TCA scenarios but avoid in QRS-widened patients. Follow institutional toxicology protocols.
- ★POST-OP DELIRIUM: scopolamine-patch + benzodiazepine + opioid + elderly = cocktail for central anticholinergic syndrome. Physostigmine 1–2 mg IV is diagnostic-and-therapeutic; rapid reversal of confusion within minutes.
- ★BRADYCARDIA RISK: have atropine drawn up before giving physostigmine for any indication. The muscarinic effect can produce profound bradycardia that requires immediate rescue.
Other drugs in Anticholinesterases
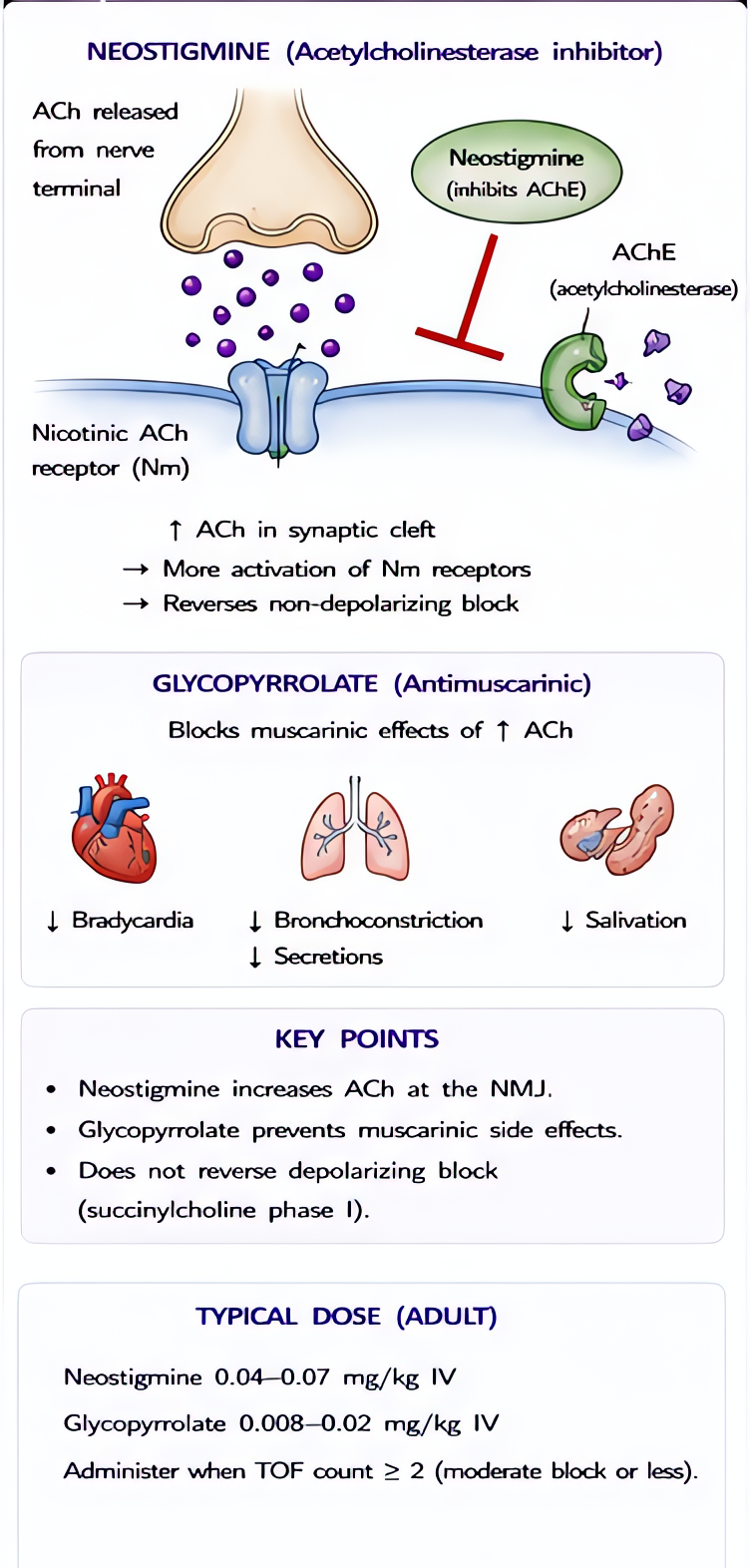
- Neostigmine
Reversibly inhibits AChE → ↑ACh at NMJ → outcompetes non-depolarizing relaxants. Co-administer antimuscarinic (glycopyrrolate or atropine) to block muscarinic side effects.
- Pyridostigmine
Reversibly inhibits acetylcholinesterase → ↑acetylcholine at the neuromuscular junction. Quaternary ammonium → does NOT cross BBB → no CNS effects. Longer-acting than neostigmine; mainstay of chronic myasthenia gravis treatment.
- Edrophonium
Reversible AChE inhibitor with the FASTEST onset (1–2 min) and SHORTEST duration (5–10 min) of the anticholinesterases. Quaternary structure → no CNS penetration. Largely historical; replaced by sugammadex in NMB reversal and by serologic AChR antibody testing in myasthenia diagnosis.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert