Ketorolac
Toradol
Non-selective NSAID (COX-1/COX-2 inhibitor)
Inhibits cyclooxygenase → ↓ prostaglandin synthesis → anti-inflammatory + analgesic + antipyretic.
Indications
- •Moderate-to-severe acute pain (typically post-op)
- •Multimodal analgesia adjunct (opioid-sparing)
- •Renal colic
- •Migraine
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Adult IV/IM (<65 yo, normal renal) | 30 mg IV/IM single dose; or 30 mg q6h (max 5 days) | — |
| Adult IV/IM (≥65 yo, <50 kg, or impaired renal) | 15 mg IV/IM q6h | — |
| Pediatric (≥2 yo) | — | 0.5 mg/kg IV q6h, max 30 mg/dose |
| Oral (after IV transition) | 10 mg PO q4-6h, max 40 mg/day | — |
Pharmacokinetics
Onset 10 min IV; peak analgesia ~2 hr; duration 4-6 hr; half-life 4-6 hr; renal excretion.
Side effects
- !GI bleed / ulceration (esp. if combined with steroids, anticoagulants, or alcohol)
- !Acute kidney injury (esp. dehydration, ACEi/ARB, elderly, baseline CKD)
- !Platelet dysfunction (reversible — duration 24-48 hr; impacts bleeding for surgical sites)
- !Bronchospasm (aspirin-exacerbated respiratory disease)
- !Increased CV risk (MI, CVA) with prolonged use
Contraindications
- ×Aspirin/NSAID allergy or AERD (Samter triad)
- ×Active GI bleed or peptic ulcer
- ×Renal impairment (CrCl <30) or volume depletion
- ×Pre-op or intraop with high bleeding-risk surgery (ENT, neurosurgery, plastic flap)
- ×Asthma with NSAID-sensitivity
- ×Late pregnancy (premature ductus closure)
- ×Anticoagulation (relative — discuss with surgeon)
Clinical pearls
- ★5-DAY MAXIMUM courtesy of FDA label: GI + renal toxicity climbs after that. Switch to oral NSAID or non-NSAID.
- ★OPIOID-SPARING: 30 mg ketorolac IV ≈ 12 mg morphine for many post-op surgeries; reduces opioid requirement 25-50%.
- ★BLEEDING SURGERY: surgeon discussion mandatory. Most ENT, plastic flap, and spine surgeons prefer no NSAID for 7-14 days. Cardiac surgery: avoid first 7 days.
- ★DEHYDRATED + ACEi PATIENT = TRIPLE-WHAMMY → AKI risk high. Hydrate well, hold ketorolac if creatinine bumps.
- ★ALTERNATIVES: IV acetaminophen (no bleeding/renal risk, weaker), celecoxib (less GI but same CV risk), gabapentinoids.
Other drugs in Narcotics & Analgesics
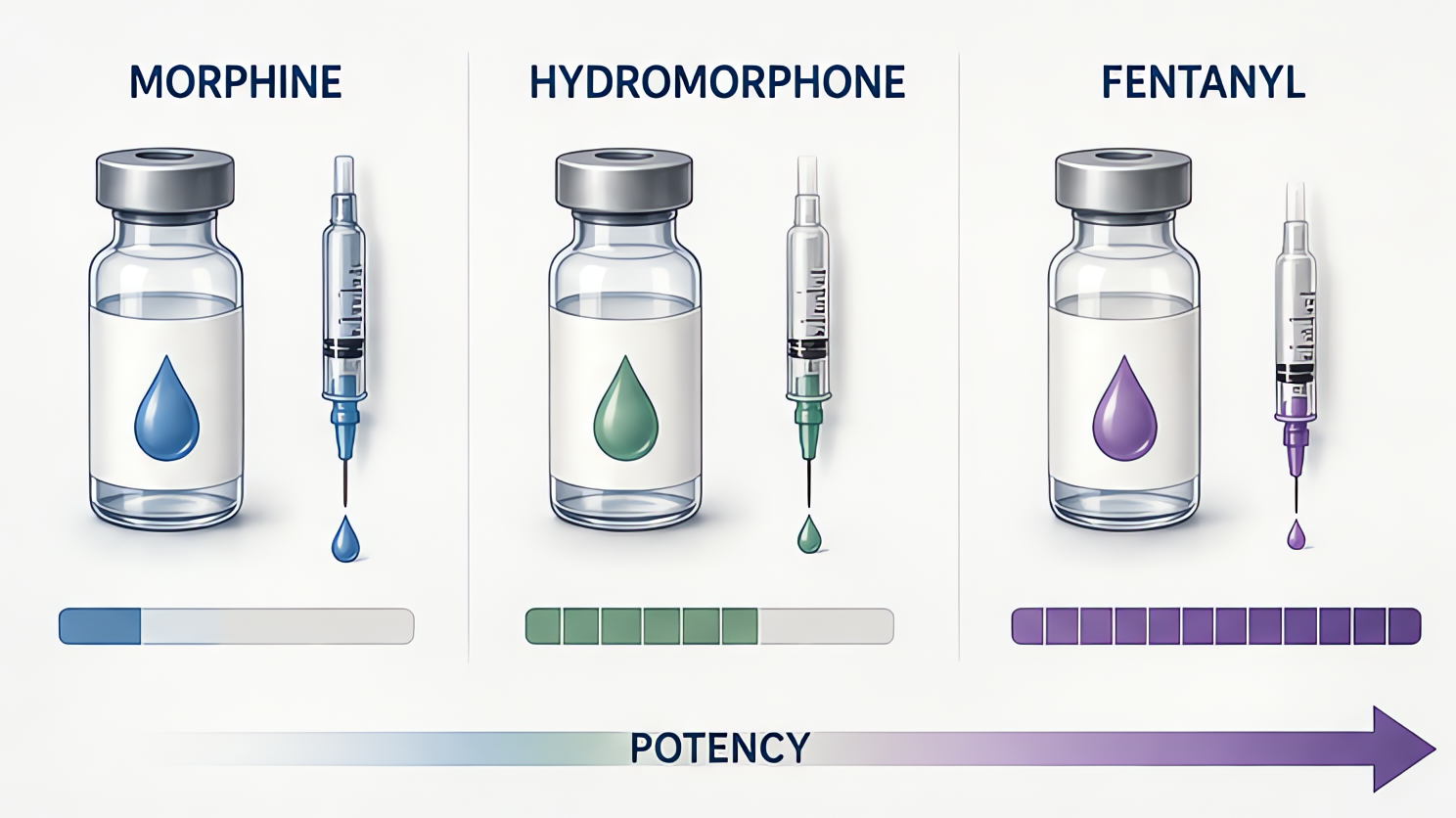
- Fentanyl
μ-opioid receptor agonist. ~100× potency of morphine.
- Remifentanil
μ-opioid agonist. Ester linkage hydrolyzed by nonspecific tissue + plasma esterases — no organ-dependent clearance.
- Morphine
μ-opioid receptor agonist. Active metabolite morphine-6-glucuronide (M6G) is analgesic and renally cleared — accumulates in renal failure → prolonged sedation/respiratory depression. Causes histamine release.
- Hydromorphone
μ-opioid agonist ~5–7× more potent than morphine. No clinically significant active metabolites → safer than morphine in renal failure. Less histamine release.
- Sufentanil
Most potent opioid in common clinical use — ~1000× morphine, ~10× fentanyl. High lipid solubility.
- Alfentanil
μ-opioid agonist ~1/5–1/10 the potency of fentanyl but FASTEST onset of the family — low pKa means a high non-ionized fraction at physiologic pH.
- Meperidine
μ-opioid agonist ~1/10 morphine, plus κ-agonism (anti-shivering). Active metabolite normeperidine is renally cleared, proconvulsant, and neurotoxic.
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert