Fentanyl
Sublimaze
Synthetic phenylpiperidine opioid agonist (μ)
μ-opioid receptor agonist. ~100× potency of morphine.
Indications
- •Intraop analgesia
- •Pre-induction blunting of laryngoscopy response
- •Postop pain
- •Patches for chronic pain
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Induction adjunct | 1–3 mcg/kg IV | 1–3 mcg/kg IV (full-term + older) |
| Intraop bolus | 0.5–1 mcg/kg IV q30 min | 0.5–1 mcg/kg IV q30 min |
| Cardiac induction | 5–25 mcg/kg IV | 5–25 mcg/kg IV (peds cardiac) |
| PCA | 10–25 mcg q5–10 min | 0.25–0.5 mcg/kg q10–15 min (age-appropriate) |
| Epidural | 1–2 mcg/mL infusion adjunct | — |
| Continuous infusion (NICU/PICU) | — | 0.5–2 mcg/kg/hr (neonates: 0.5–1 mcg/kg/hr; older: up to 2) |
Pharmacokinetics
Onset 1–2 min. Duration 30–60 min (bolus). Context-sensitive half-time ↑ with prolonged infusion.
Hemodynamic effects
Minimal at typical doses. Bradycardia at high doses.
Respiratory effects
Dose-dependent respiratory depression. Chest wall rigidity at rapid high doses (treat with NMBA).
Side effects
- !Respiratory depression
- !Pruritus
- !Nausea
- !Constipation
- !Tolerance + opioid-induced hyperalgesia at high cumulative doses
Contraindications
- ×MAOI use within 14 days (relative)
Clinical pearls
- ★Multimodal analgesia (acetaminophen, NSAID, regional, ketamine) reduces fentanyl needs and OIH.
- ★Watch for 'fentanyl chest wall' rigidity — usually with ≥ 5 mcg/kg push.
Other drugs in Narcotics & Analgesics
- Remifentanil
μ-opioid agonist. Ester linkage hydrolyzed by nonspecific tissue + plasma esterases — no organ-dependent clearance.
- Morphine
μ-opioid receptor agonist. Active metabolite morphine-6-glucuronide (M6G) is analgesic and renally cleared — accumulates in renal failure → prolonged sedation/respiratory depression. Causes histamine release.
- Hydromorphone
μ-opioid agonist ~5–7× more potent than morphine. No clinically significant active metabolites → safer than morphine in renal failure. Less histamine release.
- Sufentanil
Most potent opioid in common clinical use — ~1000× morphine, ~10× fentanyl. High lipid solubility.
- Alfentanil
μ-opioid agonist ~1/5–1/10 the potency of fentanyl but FASTEST onset of the family — low pKa means a high non-ionized fraction at physiologic pH.
- Meperidine
μ-opioid agonist ~1/10 morphine, plus κ-agonism (anti-shivering). Active metabolite normeperidine is renally cleared, proconvulsant, and neurotoxic.
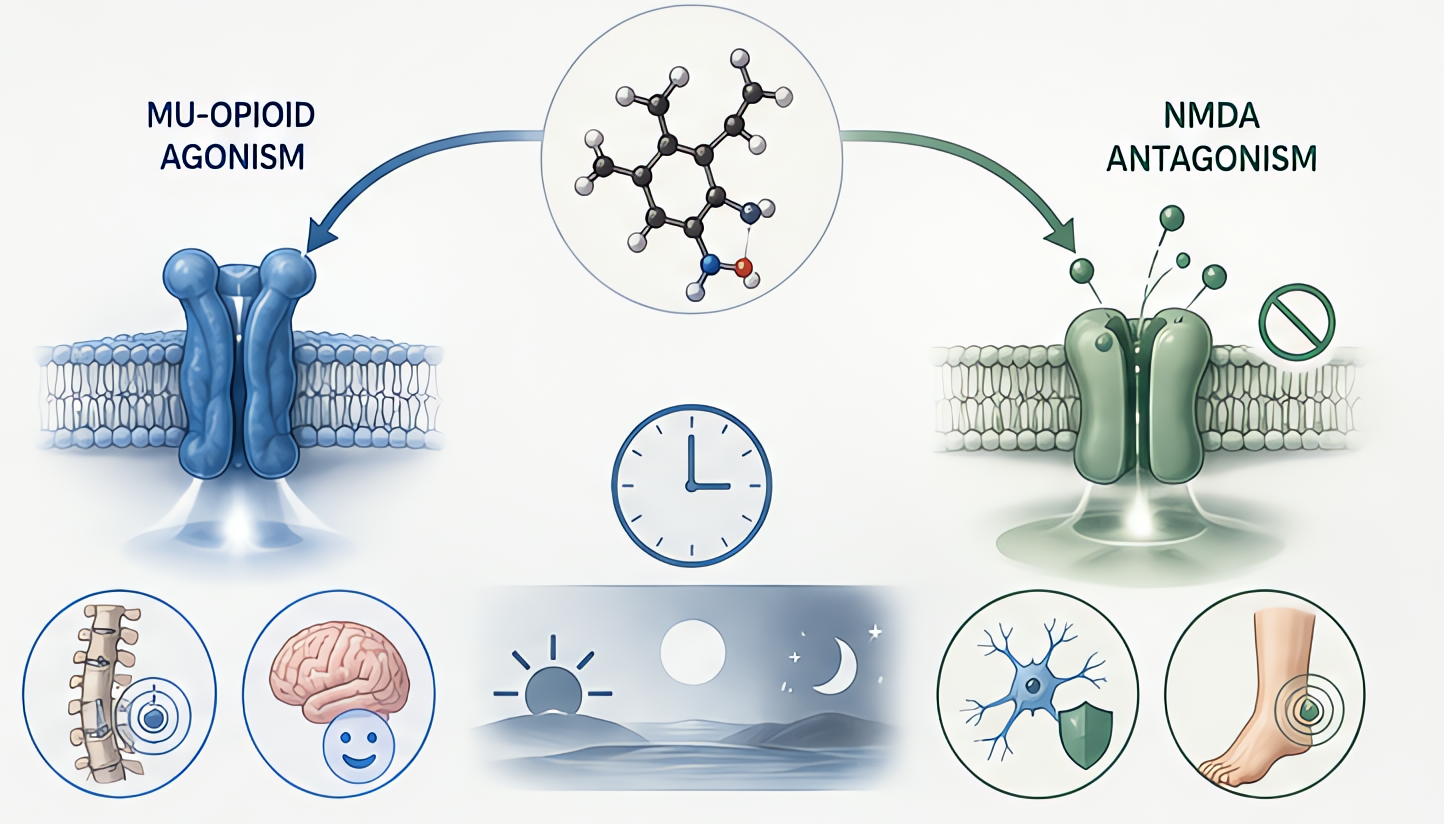
- Methadone
μ-opioid agonist with NMDA-receptor antagonism (blunts tolerance + opioid-induced hyperalgesia) and monoamine reuptake inhibition. Very long, variable half-life.
- Nalbuphine
κ-receptor agonist + μ-receptor antagonist. Ceiling on respiratory depression. Reverses μ-mediated pruritus/respiratory depression while preserving some analgesia.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Coté, A Practice of Anesthesia for Infants and Children, 7e
- •FDA package insert