Naloxone
Narcan · Evzio
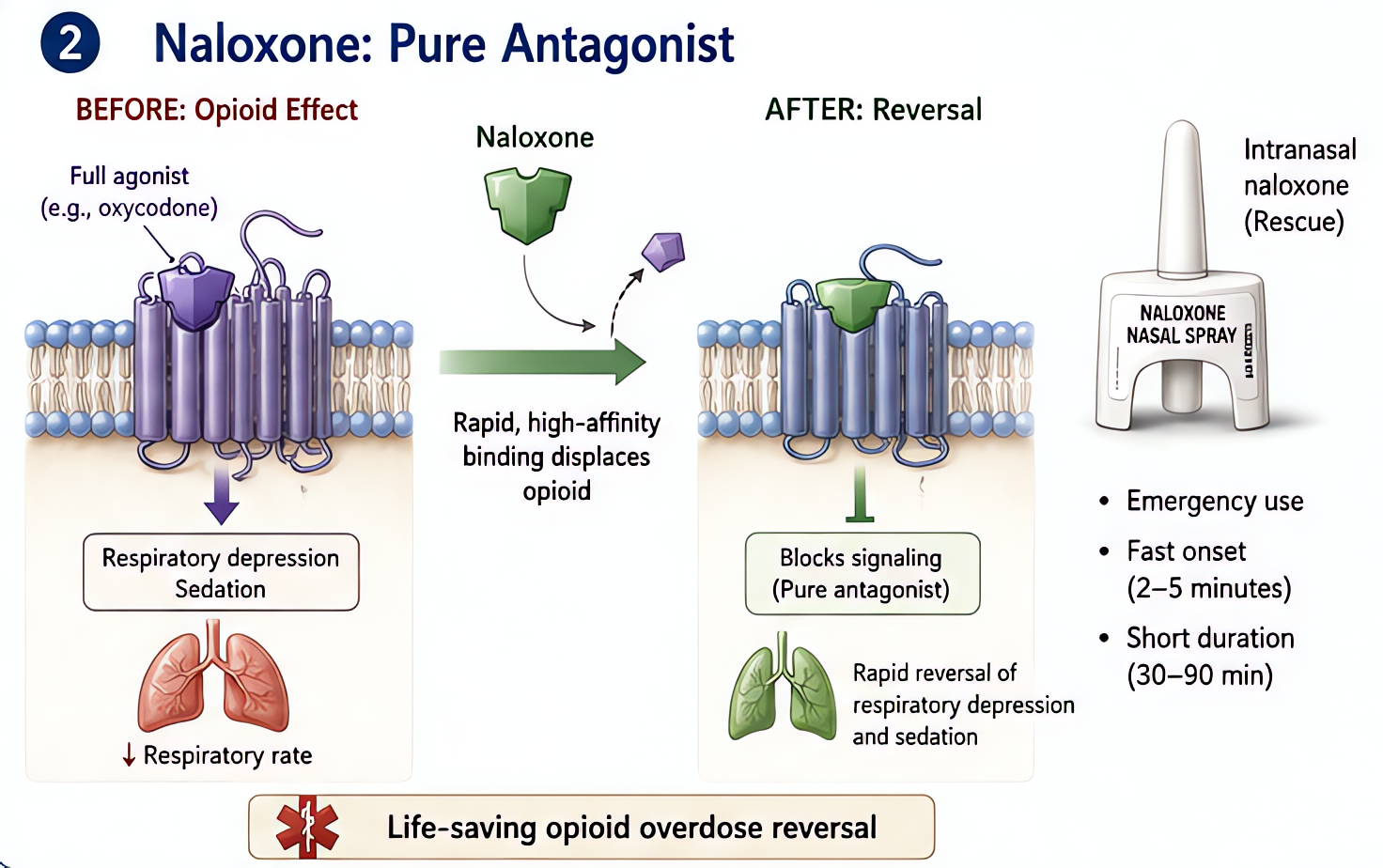
Pure mu-opioid receptor antagonist
Competitive antagonist at mu (μ), kappa, and delta opioid receptors with highest affinity for μ. Reverses respiratory depression, sedation, analgesia, miosis, pruritus, GI hypomotility from exogenous opioids.
Indications
- •Opioid overdose / respiratory depression
- •Postop respiratory depression from opioid
- •Opioid-induced pruritus (low-dose infusion)
- •Reverse fetal/neonatal depression from maternal opioid (controversial — not first-line)
- •Diagnosis of opioid intoxication
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Adult full reversal (overdose) | 0.4–2 mg IV/IM/IN q2–3 min until response or 10 mg total | — |
| Postop respiratory depression (titrated) | 40 mcg IV q1–2 min (dilute 0.4 mg in 10 mL = 40 mcg/mL) — preserve analgesia while restoring respiration | — |
| Pediatric overdose | 0.01 mg/kg IV (adult dose if >5 yr or >20 kg) | |
| Pruritus from neuraxial morphine | 1–4 mcg/kg/h IV infusion (very low dose preserves analgesia) | — |
| Intranasal community use | 4 mg IN (one Narcan nasal spray) q2–3 min | — |
Pharmacokinetics
Onset 1–2 min IV, 2–5 min IM/IN. Duration 30–60 min — IMPORTANT: shorter than most opioids → rebound respiratory depression risk (re-narcotization). Hepatic glucuronidation, renal excretion.
Hemodynamic effects
Minimal direct cardiac effect at therapeutic doses. SUDDEN COMPLETE REVERSAL can cause acute hypertension, tachycardia, pulmonary edema, arrhythmias from sympathetic surge — titrate slowly.
Respiratory effects
Restores opioid-suppressed ventilation; may unmask underlying causes of respiratory failure.
Side effects
- !Acute opioid withdrawal syndrome (dependent patients): pain, sweating, agitation, vomiting, diarrhea, hypertension
- !Pulmonary edema (sudden sympathetic surge in healthy patients with overdose)
- !Re-narcotization when naloxone wears off but opioid remains
- !Reversal of analgesia → severe acute pain
- !Seizures (rare, severe overdose)
Contraindications
- ×Hypersensitivity
Clinical pearls
- ★POSTOP TITRATION: dilute 0.4 mg in 10 mL → give 40 mcg q1–2 min until respiratory rate adequate. Restores breathing while preserving most analgesia. Full 0.4 mg bolus = pain crisis + cardiovascular surge.
- ★ALWAYS CONTINUE MONITORING after naloxone — re-narcotization at 30–60 min as naloxone wears off but long-acting opioid (morphine, hydromorphone) persists. Consider infusion 0.04–0.16 mg/h.
- ★Long-acting opioids (methadone, sustained-release morphine, fentanyl patch): may need naloxone INFUSION for hours.
- ★Chronic opioid users: small doses; risk of severe withdrawal. Goal = restore breathing, NOT zero opioid effect.
- ★Newborns with maternal opioid exposure: NO routine naloxone (NRP 2015) — supportive ventilation preferred. Naloxone may precipitate neonatal seizures in opioid-dependent infants.
Other drugs in Narcotic Reversals
- Naltrexone
Competitive antagonist at μ, κ, δ opioid receptors. Long half-life makes it useful for opioid use disorder maintenance — but poses major perioperative challenges if patients with chronic naltrexone need opioid analgesia.
- Methylnaltrexone
Quaternary derivative of naltrexone — does NOT cross the blood-brain barrier. Reverses peripheral opioid effects (constipation, urinary retention, pruritus) without antagonizing central analgesia.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert