Sevoflurane
Ultane · Sevorane
Halogenated methyl isopropyl ether — volatile general anesthetic
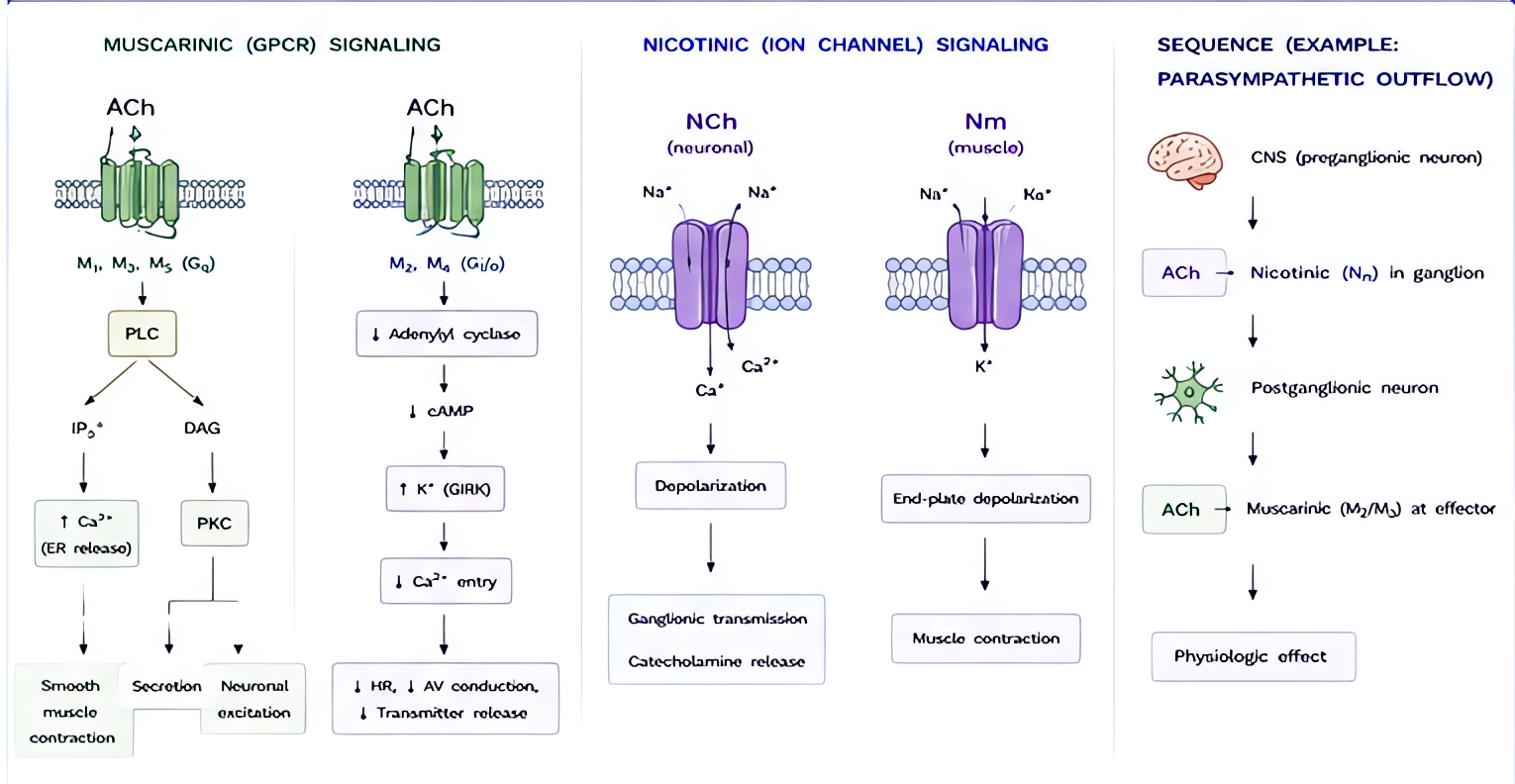
Multi-site CNS depression: GABA-A potentiation, glycine receptor potentiation, NMDA + nicotinic ACh inhibition, two-pore K⁺ channel activation. Net: dose-dependent unconsciousness, amnesia, immobility, and analgesia (modest).
Indications
- •GA induction (mask, especially pediatric)
- •GA maintenance
- •Bronchospasm rescue (volatile bronchodilation)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Mask induction (peds) | Up to 8% inspired with O₂ ± N₂O; titrate down post-LOC | 8% inspired (single-breath or stepwise) — tolerated due to non-pungent character |
| Adult induction (slow) | Stepwise 1→8% over several breaths; bridge to IV induction more common in adults | — |
| Maintenance | 0.5–2.5% inspired (1 MAC ≈ 2.05% age 40; declines ~6%/decade) | MAC age 1–6 mo ≈ 3.2%; MAC neonate ≈ 3.3%; declines to ~2.5% through childhood |
Pharmacokinetics
Blood:gas partition coefficient 0.65 (low → fast on/off). MAC 2.05% age 40, drops ~6% per decade. Minimally metabolized (~5% by CYP2E1 to inorganic fluoride + hexafluoroisopropanol). Standard wash-in/wash-out within minutes.
Hemodynamic effects
Dose-dependent ↓SVR + ↓MAP (mild–moderate). Cardiac output relatively preserved vs other volatiles. Minimal coronary vasodilation (no clinically significant 'coronary steal'). HR usually stable; can rise mildly at >1.5 MAC.
Respiratory effects
Non-pungent — gold standard for pediatric mask induction. Dose-dependent ↓TV and ↑RR (rapid shallow). Bronchodilator. Blunts hypoxic + hypercarbic ventilatory drive.
Side effects
- !Compound A formation in CO₂ absorbents (esp. desiccated soda lime with NaOH/KOH bases) — theoretical nephrotoxicity at FGF <1 L/min × prolonged exposure; modern Amsorb-class absorbents eliminate. Clinical relevance in humans remains unproven.
- !Emergence delirium in pediatric patients (20–80% incidence; mitigate with dexmedetomidine 0.3 mcg/kg, propofol 1 mg/kg at end, or fentanyl)
- !MH trigger (all halogenated agents are)
- !Postoperative shivering (volatile-class effect)
- !Mild hepatotoxicity (rare; lower than des/iso/halothane)
Contraindications
- ×MH susceptibility (any volatile)
- ×Severe hepatic dysfunction (relative)
- ×Pheochromocytoma (relative — sympathetic stim with high-dose volatiles)
Clinical pearls
- ★FAST induction + FAST emergence: blood:gas 0.65 means changes in inspired concentration reach effect-site within 1–2 min.
- ★Pediatric induction of choice — non-pungent, no breath-holding, no laryngospasm trigger like desflurane.
- ★MAC additive with N₂O: 1 MAC sevo (2.05%) + 50% N₂O (≈ 0.48 MAC) = ~1.48 MAC total.
- ★Compound A is essentially a non-issue with modern (Amsorb-class) absorbents and FGF >1 L/min.
- ★Avoid for 'awake-craniotomy asleep phases' — emergence delirium worse than propofol TIVA.
Other drugs in Inhalation Agents
- Desflurane
Same multi-site mechanism as sevoflurane: GABA-A + glycine potentiation, NMDA + nicotinic ACh inhibition, K⁺ channel activation.
- Isoflurane
Volatile anesthetic. Multiple sites: potentiates GABA-A, antagonizes NMDA, activates two-pore-domain K⁺ channels, modulates glycine. Lower potency than sevoflurane but produces deeper unconsciousness per MAC. Pungent — not used for inhalation induction.
- Nitrous Oxide
NMDA-receptor antagonism (primary) + opioid/GABA effects → analgesia + amnesia. Weak anesthetic (MAC 104%) so used as an adjuvant, not a sole agent.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert