Acetazolamide
Diamox
Carbonic anhydrase inhibitor
Reversibly inhibits carbonic anhydrase in proximal renal tubule, choroid plexus, ciliary body, RBC. Renal effect: ↓Na/H exchange → bicarbonate diuresis + mild Na/water loss + metabolic acidosis. CNS effect: ↓CSF production. Eye effect: ↓aqueous humor.
Indications
- •Acute mountain sickness prophylaxis and treatment
- •Glaucoma — open-angle and acute angle-closure (adjunct)
- •Pseudotumor cerebri / idiopathic intracranial hypertension
- •Metabolic alkalosis from prolonged diuretic use
- •Refractory CHF (synergy with loop diuretic)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| AMS prophylaxis | 125–250 mg PO bid starting 24 h before ascent | — |
| Glaucoma | 250 mg PO qid; 500 mg IV in acute closure | — |
| Metabolic alkalosis correction | 250–500 mg IV/PO daily × 1–3 days | — |
| Pseudotumor cerebri | 500–1000 mg PO bid (titrated) | — |
Pharmacokinetics
Onset 1–2 h PO, minutes IV. Duration 8–12 h. Renal excretion unchanged.
Hemodynamic effects
Mild diuretic — minimal hemodynamic effect at usual doses.
Respiratory effects
Mild metabolic acidosis → compensatory hyperventilation; basis for AMS efficacy (acclimatization-mimicking).
Side effects
- !Metabolic acidosis (the mechanism — useful for AMS, problematic in COPD)
- !Paresthesias (tingling fingertips/lips, very common)
- !Hypokalemia
- !Renal stones (alkaline urine + low citrate)
- !Sulfa hypersensitivity (cross-reactive with sulfa antibiotics)
- !Aplastic anemia (rare, idiosyncratic)
Contraindications
- ×Sulfa allergy (relative — most patients tolerate)
- ×Severe hepatic disease (hepatic encephalopathy)
- ×Severe renal failure
- ×Adrenocortical insufficiency
- ×Hyponatremia / hypokalemia uncorrected
Clinical pearls
- ★AMS PHARMACOLOGIC ANALOG OF ACCLIMATIZATION: induces metabolic acidosis → respiratory drive boost → better high-altitude oxygenation. 125 mg bid starting 24 h before ascent is the validated regimen.
- ★PARESTHESIAS = NORMAL: 'pins and needles' in fingertips and around the mouth is so common it's reassuring — confirms the drug is on board. Counsel patients in advance.
- ★ICP / PSEUDOTUMOR: useful adjunct because it reduces CSF production at the choroid plexus. Less common in modern practice (topiramate often preferred for IIH).
- ★PERIOPERATIVE: chronic acetazolamide users arrive with mild metabolic acidosis. ABG interpretation in these patients should account for that — don't 'fix' a chronic adaptation.
Other drugs in Diuretics
- Furosemide
Inhibits the Na-K-2Cl cotransporter in the thick ascending loop of Henle. Massive natriuresis + kaliuresis + magnesiuresis. Also a venodilator — drops preload within minutes, before diuresis kicks in.
- Mannitol
Freely filtered, not reabsorbed. Pulls water from tissues into vascular space (transient ↑intravascular volume) then drives osmotic diuresis. Reduces ICP by drawing water across an intact blood-brain barrier.
- Spironolactone
Competitive antagonist at the mineralocorticoid receptor in the distal nephron → inhibits aldosterone-mediated Na reabsorption + K secretion. Net effect: mild Na/water loss + K retention + Mg retention. Also a weak androgen-receptor antagonist.
- Bumetanide
Inhibits the Na-K-2Cl cotransporter in the thick ascending limb → potent diuresis. ~40× more potent than furosemide (1 mg bumetanide ≈ 40 mg furosemide).
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert
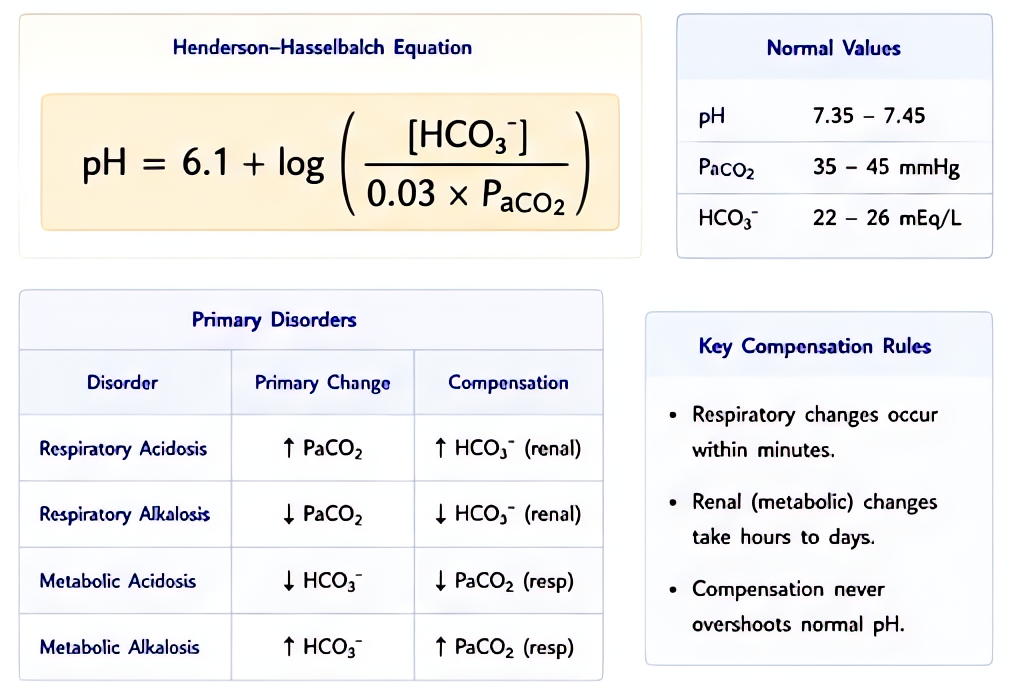
![Acid-base electrolytes Henderson-Hasselbalch: pH = pKa + log[HCO3-/(0.03 x PaCO2)]. Metabolic acidosis decreased HCO3 (kidneys, metabolic), respiratory acidosis increased PaCO2 (lungs). Compensation c](https://pfcaitzjiuhtyrjwevzj.supabase.co/storage/v1/object/sign/manual-panels/3312e4bd-b0ee-4c78-89df-8279838bfaf9.png?token=eyJraWQiOiJzdG9yYWdlLXVybC1zaWduaW5nLWtleV82NWQ1NTMxOC1iZWMzLTQxY2MtOGVhMC1lZjNhNjY5ZGU5M2IiLCJhbGciOiJIUzI1NiJ9.eyJ1cmwiOiJtYW51YWwtcGFuZWxzLzMzMTJlNGJkLWIwZWUtNGM3OC04OWRmLTgyNzk4MzhiZmFmOS5wbmciLCJzY29wZSI6ImRvd25sb2FkIiwiaWF0IjoxNzg1ODY2MDQxLCJleHAiOjE3ODU4Njk2NDF9.MRjQf4nrOOLRvCJP1jqJwSovRdZ7fnIwPnxn-9wUfSc)