Scopolamine
Transderm-Scop
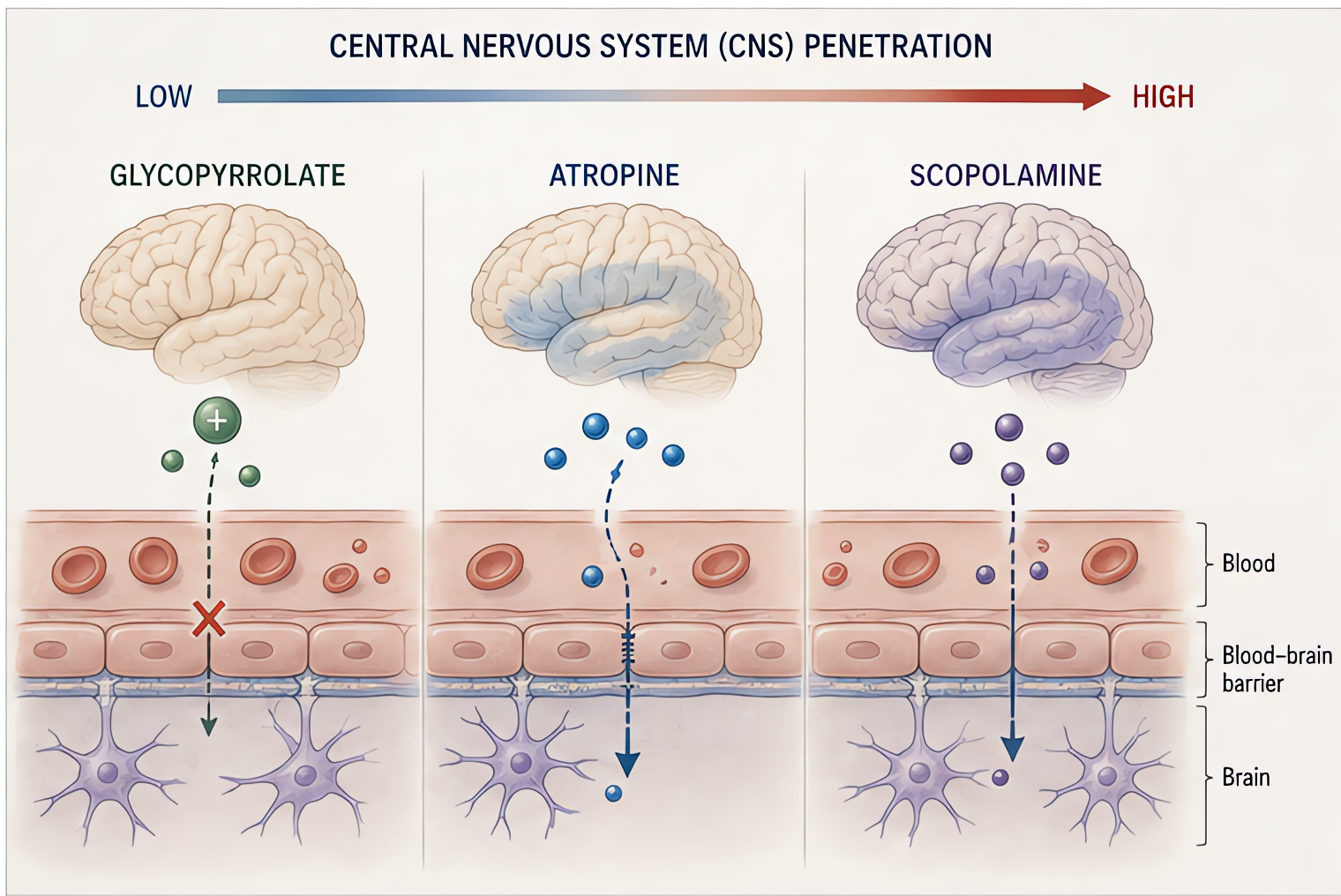
Tertiary-amine muscarinic antagonist (CNS-active)
Competitive muscarinic antagonist with high CNS penetration. Strong central antiemetic + amnestic effects via vestibular nuclei + chemoreceptor trigger zone. Weak peripheral effects compared with atropine.
Indications
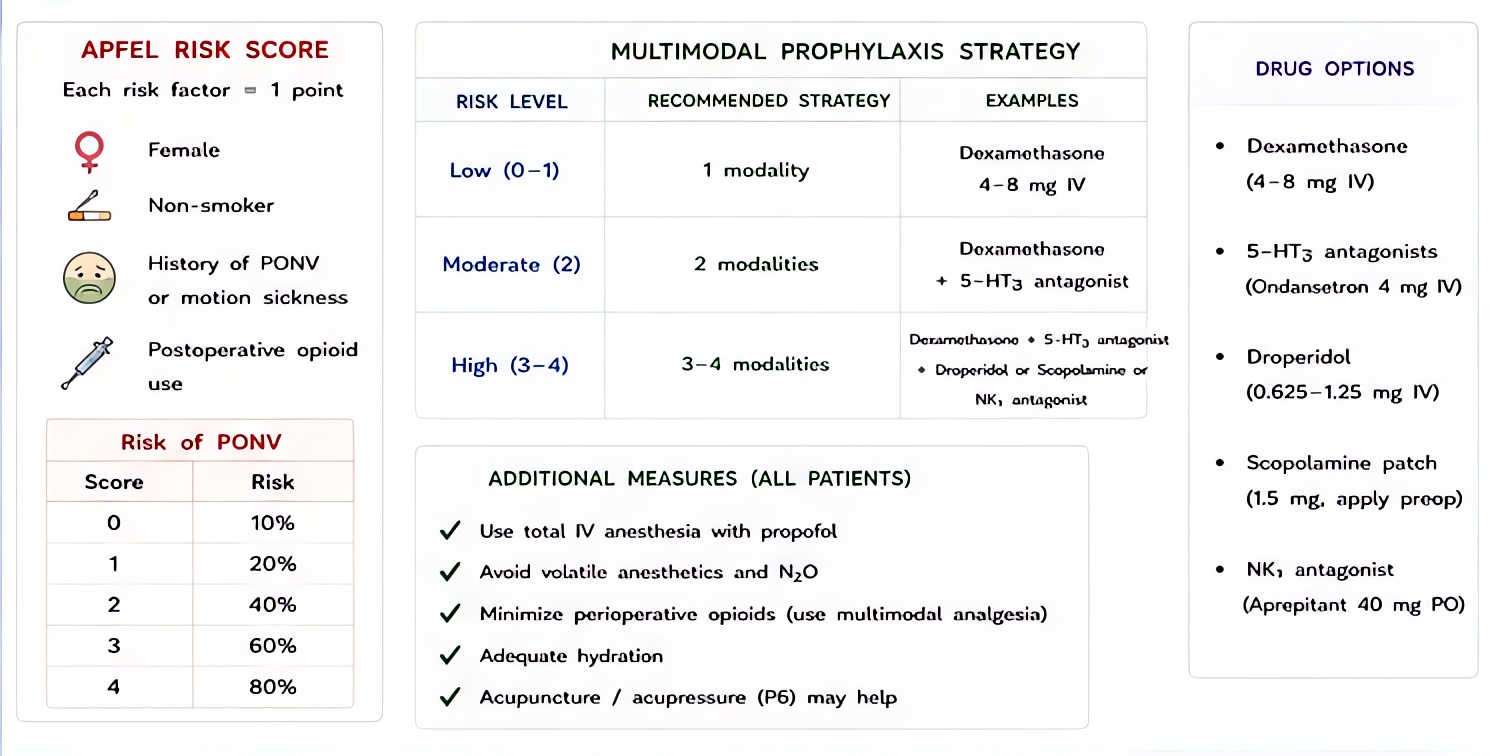
- •PONV prophylaxis (especially for high-risk: female, non-smoker, motion-sickness history, opioids planned)
- •Motion sickness prevention
- •Antisialagogue (rarely first-line)
- •End-of-life secretion management
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| PONV patch | 1.5 mg transdermal patch behind the ear, applied evening before surgery (4-h onset; 72-h duration) | — |
| PONV IV | 0.2–0.4 mg IV (rarely used; patch preferred) | — |
Pharmacokinetics
Patch onset 4 h, peak 24 h, duration 72 h after removal. Hepatic metabolism. Crosses BBB freely.
Hemodynamic effects
Minimal at clinical doses.
Respiratory effects
Mild bronchodilation; secretion-drying.
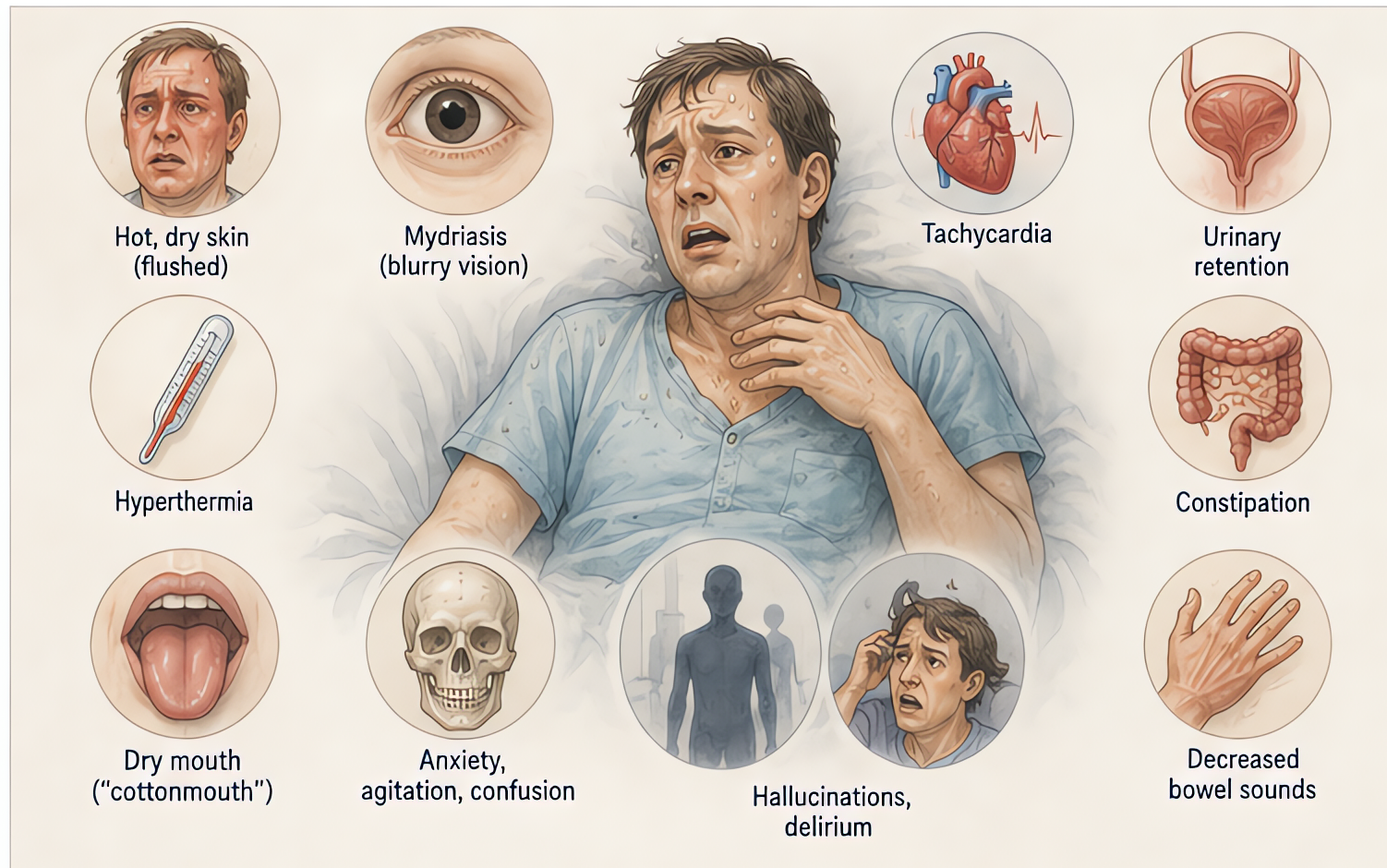
Side effects
- !Sedation, confusion, delirium — especially elderly. Most common reason for early removal.
- !Dry mouth
- !Mydriasis + cycloplegia — caution narrow-angle glaucoma; pupil asymmetry from finger contamination is a documented misread as cranial-nerve event
- !Urinary retention
- !Withdrawal symptoms after 72-h patch (dizziness, nausea, headache)
Contraindications
- ×Narrow-angle glaucoma
- ×Severe hepatic/renal impairment
- ×Pregnancy (Category C — risk vs benefit)
- ×Pyloric obstruction
Clinical pearls
- ★PUPIL TRAP: hand-to-eye contamination after handling patch causes unilateral mydriasis that can be mistaken for stroke / herniation. Always wash hands after patch placement.
- ★ELDERLY: use sparingly. Anticholinergic load + sedation can produce postoperative delirium that lasts days.
- ★PATCH TIMING: place evening before for AM cases. 4-h onset means same-day placement misses peak effect.
- ★COMBINE: synergistic with ondansetron + dexamethasone for high-risk PONV (Apfel ≥3).
Other drugs in Anticholinergics
- Glycopyrrolate
Competitive antagonist at peripheral muscarinic acetylcholine receptors. Quaternary structure → does NOT cross blood-brain barrier (unlike atropine, scopolamine) → no CNS effects. Primary anesthesia uses: (1) prevent muscarinic effects of anticholinesterases during NMB reversal; (2) reduce secretions before fiberoptic/awake intubation.
- Atropine
Competitive antagonist at muscarinic ACh receptors. Tertiary amine → CROSSES blood-brain barrier (in contrast to glycopyrrolate) → central anticholinergic effects possible. Faster onset than glycopyrrolate; useful for emergent bradycardia.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert