Phenoxybenzamine (Dibenzyline)
Dibenzyline
Non-competitive irreversible alpha-1 + alpha-2 antagonist
IRREVERSIBLE non-competitive antagonist at alpha-1 + alpha-2 adrenergic receptors. Covalently binds + permanently inactivates receptors — duration of action depends on receptor RESYNTHESIS (24-48 h after each dose). Distinguishes from competitive antagonists (phentolamine) where catecholamine surge can overcome blockade.
Indications
- •Pheochromocytoma — preoperative alpha blockade (preferred over selective α1 like prazosin in many centers — though doxazosin/prazosin also acceptable per Endocrine Society 2014)
- •Neurogenic bladder hypertonia (off-label)
- •Raynaud phenomenon (rarely used)
Dosing
| Context | Adult | Pediatric |
|---|---|---|
| Pheo preop alpha blockade | 10 mg PO BID, increase by 10-20 mg/day every 2-3 days; titrate to mild postural hypotension + nasal stuffiness + target HR 70-80 sitting; typical effective 40-100 mg/day; START ≥7-14 days preop | — |
Pharmacokinetics
Onset 2 h. Duration of effect 24-48 h per dose (irreversible — depends on receptor resynthesis). Hepatic metabolism.
Hemodynamic effects
↓BP (especially upright — postural hypotension common + intentional). Reflex tachycardia. After alpha blockade established → liberal salt + fluid → 'fill the contracted intravascular space' before surgery.
Side effects
- !Postural hypotension (intended endpoint of titration)
- !Reflex tachycardia (add beta-blocker AFTER alpha block established — never before)
- !Nasal congestion
- !Sedation
- !Inhibition of ejaculation
- !Miosis
Contraindications
- ×Hypersensitivity
- ×Active hypotension
Clinical pearls
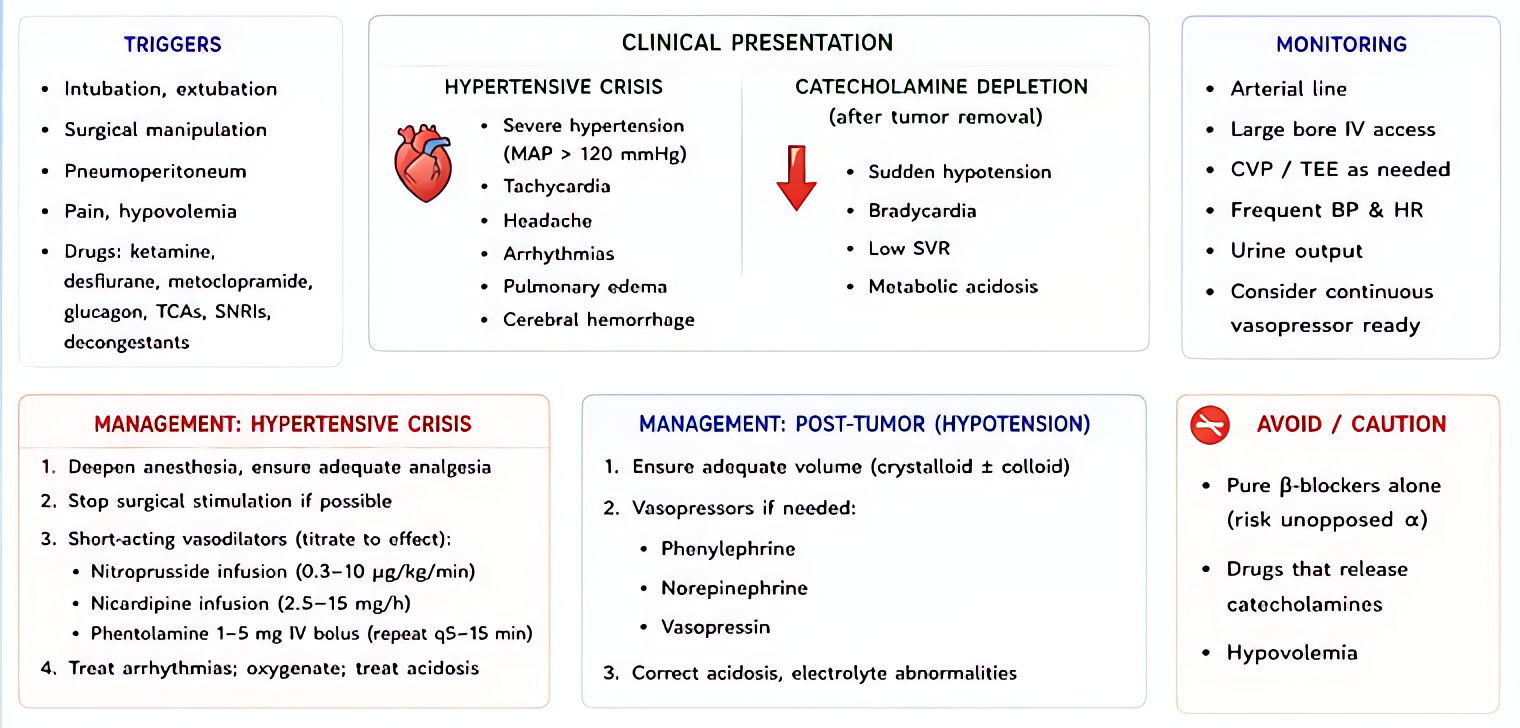
- ★PHEO PROTOCOL: alpha blockade ≥7-14 days preop (target endpoints: orthostatic hypotension + nasal congestion + target HR sitting); LIBERAL SALT + FLUID intake (counters volume contraction); ADD BETA-BLOCKADE only AFTER alpha (unopposed beta + intact alpha = severe HTN crisis + reflex bradycardia + arrest).
- ★ALTERNATIVE: doxazosin or prazosin (selective α1, competitive — easier titration but possibly less reliable blockade for surgery — Endocrine Society 2014 considers both acceptable).
- ★Postop: profound hypotension common after tumor removal (catecholamine drop + persistent alpha blockade) — vasopressor + volume support.
- ★DO NOT discontinue suddenly — wean over 1-2 weeks once tumor removed + recovery established.
Other drugs in Cardiac / BP
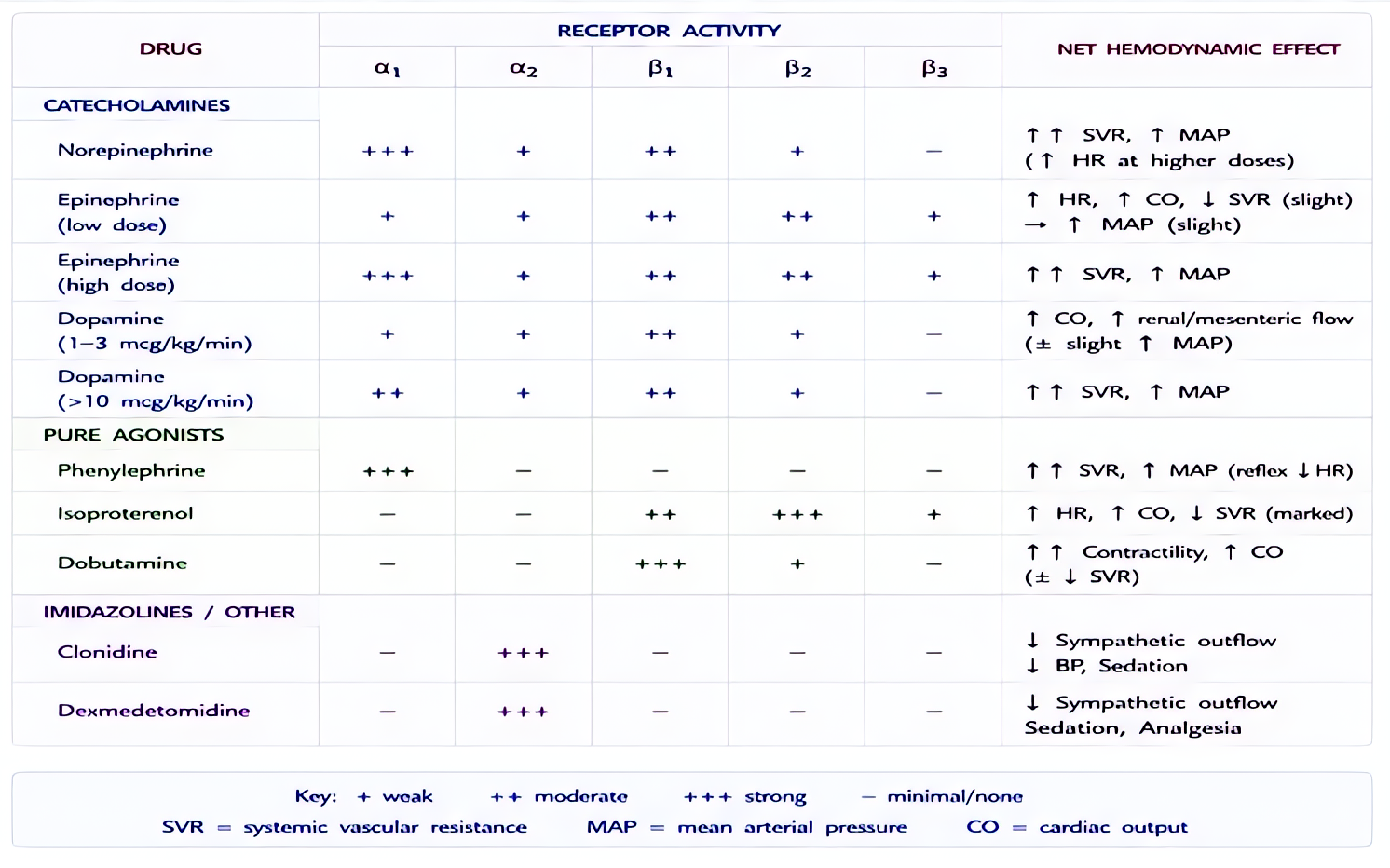
- Epinephrine
α1 (vasoconstriction), α2, β1 (inotropy + chronotropy), β2 (bronchodilation, vasodilation in skeletal muscle). Dose-dependent receptor preference: low-dose β-predominant, high-dose α-predominant.
- Norepinephrine
Strong α1 → vasoconstriction. Mild β1 → modest inotropy. Minimal β2.
- Phenylephrine
Pure α1 agonist → vasoconstriction. No β activity.
- Dexmedetomidine
α2 agonist (locus coeruleus) → sedation + analgesia + anxiolysis without significant respiratory depression.
- Vasopressin
Endogenous nonapeptide hormone. V1 receptor agonist on vascular smooth muscle (Gq → IP3 → Ca²⁺ → vasoconstriction). V2 on renal collecting ducts (Gs → cAMP → aquaporin insertion → water reabsorption). At pressor doses (0.01–0.04 U/min), V1 effects dominate.
- Esmolol
Selective β1-adrenergic receptor antagonist. Decreases HR, contractility, conduction velocity, and AV node refractoriness. Selectivity for β1 over β2 reduces (does not eliminate) bronchospasm risk vs non-selective beta-blockers.
- Magnesium Sulfate
Multiple mechanisms: (1) NMDA receptor antagonism (anticonvulsant, analgesic); (2) Voltage-gated calcium channel blockade in vascular + uterine smooth muscle (vasodilation, tocolysis); (3) Decreased ACh release at neuromuscular junction (NMB potentiation); (4) Membrane stabilization (antiarrhythmic, especially torsades).
- Amiodarone
Multichannel blockade — primarily class III (K+ channel block → prolonged repolarization, increased refractory period), plus class I (Na+ block), class II (β-blocker), class IV (Ca²⁺ block) properties. Treats most supraventricular AND ventricular arrhythmias. Long elimination half-life (weeks–months) limits chronic use.
Browse all classes: /reference/drugs
Suggested reading
- •Stoelting & Hines, Pharmacology & Physiology in Anesthetic Practice, 6e
- •Miller's Anesthesia, 9e
- •FDA package insert